Category: Business
Government Shutdown Changes

What has changed due to the Government Shutdown?
It’s pandemic-era flexibilities that will come to an end:
- Geographic restrictions that only permitted telehealth in medically underserved areas
- Requiring the patient to go to an originating site (a health care facility) instead of being in their homes
- Allowing therapists (PTs, OTs, SLPS, audiologists) to perform services via telehealth
Behavioral health via telehealth will still be allowed after September 30th, because Congress passed a law allowing it permanently. It won’t be affected by a government shutdown, if one occurs. The Social Security Act references “mental health” as opposed to “behavioral”.
Quoting the MLN Matters Article on E/M services
MLN006764 September 2025
Telehealth Services
Section 2207 of the Full-Year Continuing Appropriations and Extensions Act, 2025, extended many of these flexibilities through September 30th, 2025. Starting October 1, 2025, the statutory limitations that were in place for Medicare telehealth services before the COVID-19 public health emergency (PHE) will retake effect for most telehealth services.
These include:
- Geographic restrictions
- Location restrictions on where you can provide services
- Limitations on the scope of practitioners who can provide telehealth services
That is, telehealth as we know it to anywhere in the country, in the patient’s home ends. How do you know if you are in an underserved area, and can continue to do telehealth? Quick and easy: could your practice do telehealth before the pandemic? Yes: in all likelihood, you can continue, but remember the patient must go to an originating site, not their homes. Are you in an underserved area? Check here.
At CodingIntel, we have a copy of the CMS telehealth fact sheet from prior to the pandemic. It isn’t up-to-date with the list below, but it will tell you the rules for most practices in the country if a shutdown occurs.
Still allowed are services that weren’t implemented as a result of the pandemic.
eCFR :: 42 CFR 410.78 — Telehealth services.
(iv) The geographic requirements specified in paragraph (b)(4) of this section do not apply to the following telehealth services:
(A) Home dialysis monthly ESRD-related clinical assessment services furnished on or after January 1st, 2019, at an originating site described in paragraphs (b)(3)(vi), (ix), or (x) of this section, in accordance with section 1881(b)(3)(B) of the Act; and
(B) Services furnished on or after January 1st, 2019, for purposes of diagnosis, evaluation, or treatment of symptoms of an acute stroke.
(C) Services furnished on or after July 1st, 2019, to an individual with a substance use disorder diagnosis, for purposes of treatment of a substance use disorder or a co-occurring mental health disorder.
(D) Services furnished on or after January 1st, 2025, for the purposes of diagnosis, evaluation, and/or treatment of a mental health disorder. Payment will not be made for a telehealth service furnished under this paragraph unless the physician or practitioner has furnished an item or service in person, without the use of telehealth, for which Medicare payment was made (or would have been made if the patient were entitled to, or enrolled for, Medicare benefits at the time the item or service is furnished) within 6 months prior to the initial telehealth service and within 6 months of any subsequent telehealth service.
Betsy
UHC “Check by Member” Authorization Tool
UHC says they have a smarter way to check prior authorization requirements.
Our upgraded Check by Member tool is now the most accurate and reliable way to confirm prior authorization requirements.
- Personalized results based on member-specific data
- Same trusted source as our phone advocates
- Instant answers with no hold time

Beware of Calls Appearing to Come From TDLR
“We’ve been hearing from licensees that some of you have received suspicious phone calls that appear to come from the TDLR Customer Service line (512-463-6599).
These calls usually come from someone claiming to be a TDLR investigator who says there’s an issue with the TDLR license or file. Other calls have claimed that the person receiving the call is a victim of identity theft and that a criminal case has been filed against them. Other calls have claimed that the FBI is investigating the licensee.
Please know this: we won’t call you to tell you that your license is suspended or that you’re being investigated or ask you for money.
If you receive a phone call that appears to come from TDLR but you haven’t called or emailed us first – and if the caller is asking for personal information or requests payment – please don’t provide any information or payment. Call TDLR first to confirm whether we actually called you – because we probably didn’t.”
NEW TMB Website is Live!
The Texas Medical Board (TMB) is excited to announce that their redesigned website is now live!
They have made updates to improve our experience and ensure easier access to information and services but don’t worry, all existing systems, including My TMB, remain unchanged and fully accessible.
What’s New:
- New Website & Email Addresses: Our website has moved from tmb.state.tx.us to www.tmb.texas.gov. TMB staff and board member email addresses have also changed to the @tmb.texas.gov domain, aligning with other Texas state agencies.
- Fresh Look & Improved Navigation: The updated design features a cleaner, more modern layout with streamlined navigation to help you find what you need more easily.
Tip: Don’t forget to update any bookmarks or saved links to our new website: www.tmb.texas.gov
If you have questions about finding information on the new site, please contact the TMB Customer Service team at (512) 305-7030 or, within Texas, (800) 248-4062. You may also send an email to [email protected]
Physician NPI Revocations
The US Department of Health and Human Services will close six of its 10 regional counsel offices in 2025, raising concerns about delays, due process and physician appeals of NPI revocations.
Why does this matter to doctors? First, and most obviously, many enforcement actions could be slowed to a crawl, which would at first blush, seem to be a good thing for doctors.
However, there is a second problem. Some actions, such as “revocations” of NPI numbers, can be performed administratively, without any legal due process whatsoever. When this happens, providers may receive a letter informing them that their NPI number has been suspended or revoked together with a statement of the provider’s “appeal” rights.
Although doctors must appeal immediately, an appeal cannot go forward without lawyers from the OGC to appear on behalf of HHS. What happens if there aren’t any?
I tried a case in 2021 with a fully staffed OGC. First, to the Department Appeals Board and then to an ALJ in Washington D.C. My client’s offense? “Failure to produce medical records.” HHS administratively revoked my client’s NPI for 10 years.
While the DAB lowered the revocation to 3 years, when we appealed to the ALJ, we didn’t get an answer for two more years, during which time, the doctor was not allowed to submit any claims to CMS. And this was with a fully staffed OGC. Can you imagine what will happen with 6 of 10 offices closed?
A physician could continue to see patients, during the appeal of a suspension or revocation, but ordinarily must hold the claims until his NPI number suspension is reversed. Which, as I noted, took me two years to push an appeal through, when the OGC was fully staffed.
I have no idea how anyone is going to get any relief, if no one can have a hearing. Meaning, “due process” no longer exists in NPI revocations.
Martin Merritt is a health lawyer and health care litigator at Martin Merritt PLLC, as well as past president of the Texas Health Lawyers Association and past chairman of the Dallas Bar Association Health Law Section. He can be reached at [email protected].
Highlights for Aetna OfficeLink Updates
Claim and Code Review Program (CCRP) update
Starting December 1, you might see new claim edits
This update applies to both our commercial and Medicare members.
Beginning December 1, 2025, you may see new claim edits. These are part of our CCRP. These edits support our continuing effort to process claims accurately for our commercial, Medicare and Student Health members. You can view these edits on our provider portal on Availity.
For coding changes, go to Aetna Payer Spaces > Resources. In the search bar, search for “expanded claim edits.”
Except for Student Health, you’ll also have access to our code edit lookup tools. To find out if our new claim edits will apply to your claim, log in to Availity®. You’ll need to know your Aetna® provider ID number (PIN) to access our code edit lookup tools.
We may request medical records for certain claims, such as high-dollar claims, implant claims, anesthesia claims, and bundled services claims, to help confirm coding accuracy.
Changes to our National Precertification List (NPL)
These changes apply to our commercial and Medicare members, unless otherwise noted.
Effective January 1, 2026, we’ll require precertification for the following:
• Electrophysiological (EP) study (93654)
• Yondelis® (trabectedin, J9352)
• Docivyx™ (docetaxel, J9172) — Medicare members only
Check out the Original Publication, titles like:
- How to secure an authorization
- Urgent requests
- Changes to commercial drug lists begin on January 1
- And More
TMA Billing, Coding, and Payment Resources
TMA’s billing, coding, and payment page offers resources for physician practices, from one end of the continuum to the other. Educate yourself with our articles and tools, or get help with more complex questions.
Physician Payment Resource Center
TMA’s Physician Payment Resource Center (formerly known as the Hassle Factor Log and the Reimbursement, Review and Resolution Service) goes to bat for members by helping to resolve issues related to insurance payments.
TMA can help resolve issues with your payer network status, prompt-pay, and other reimbursement claims. Learn More
Billing and Coding Hotline
Speak directly with TMA’s certified coders and staff experts about regulatory compliance, billing and coding, payment, and licensure concerns.
(512) 370-1414
Five (5) Tips for Tightening Referrals
When a patient leaves your office with a referral slip, it should represent the start of seamless specialty care. Too often, though, the process falls apart. Patients forget to schedule, specialists never send notes back, or documentation gaps raise liability concerns. The result? Fragmented care, frustrated patients, and potential revenue leakage for your practice. By rethinking how referrals are handled, physicians and administrators can strengthen continuity of care, reduce risks, and make the process smoother for everyone involved. Here are five strategies to tighten up your referral process.
Standardize your referral protocols.
Without a consistent system, referrals can become a patchwork of individual physician habits. Establishing clear protocols, such as using a referral checklist or template, helps reduce variation and improves reliability. Standardization also supports quality initiatives and payer requirements. One practice leader told Physicians Practice that creating uniform workflows was key to making sure payers actually paid for the care provided, underscoring the financial upside of consistency
Lean into data-driven decision support
Referrals don’t have to be based on gut instinct or habit alone. Practices can use analytics to weigh outcomes data, proximity, and even HEDIS scores when deciding which specialist to send patients to. This kind of data-driven approach has been shown to reduce unnecessary costs and improve patient satisfaction.
Use AI to prescreen and prioritize requests
Artificial intelligence is starting to take on a supportive role in referral management. For example, some health systems are testing AI models that prescreen referral requests and flag the ones most likely to need urgent specialist care. That means physicians can focus attention on complex cases while routine referrals move more efficiently.
Improve communication and tracking with colleagues
Even the best referral can fail if the patient never makes the appointment—or if the referring doctor never sees the specialist’s notes. Research shows nearly a third of patients over 65 never follow through with their referrals. Better communication between practices, whether through shared EHR systems, referral dashboards, or simple follow-up calls, can close that loop.
and they’ve also pointed out that stronger collaboration between physicians can keep patients from slipping through the cracks.
Document your referral rationale thoroughly
Liability issues around referrals often stem from documentation—or the lack of it. Recording why you referred, what diagnostic steps came first, and whether you received and reviewed the specialist’s notes is crucial. Some practices use a “rule of three,” referring only after three visits without resolution, to provide consistency and documentation clarity.
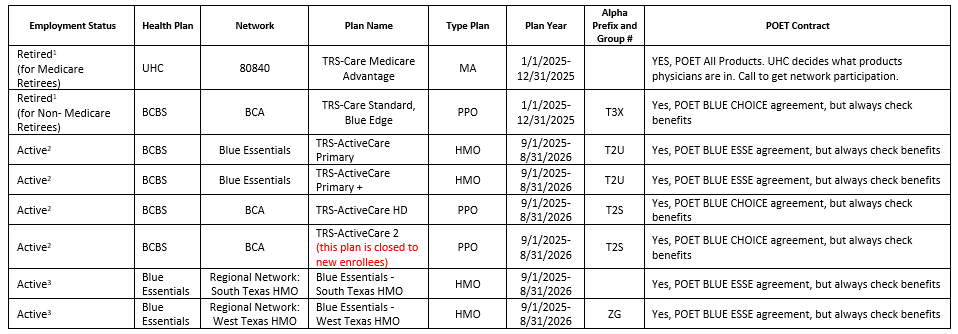
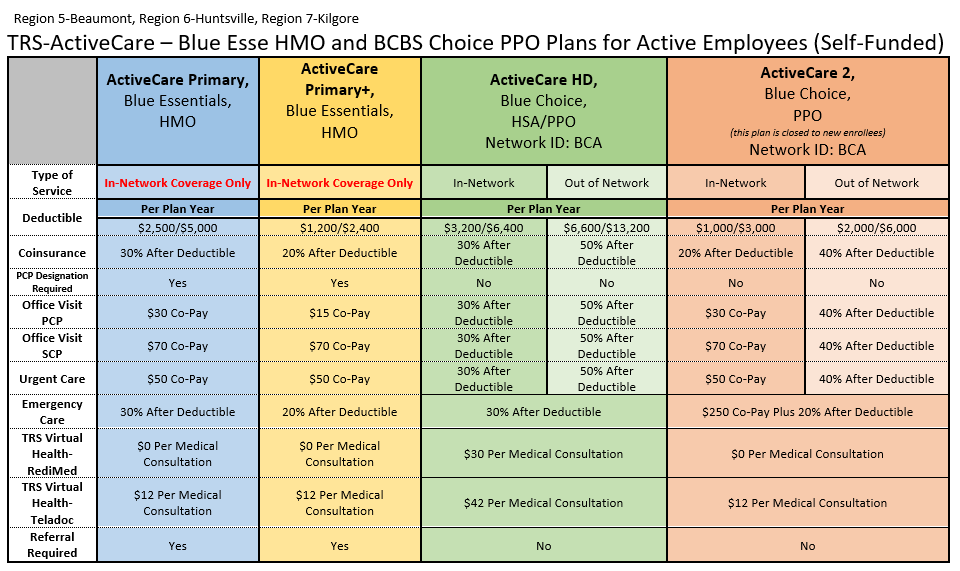
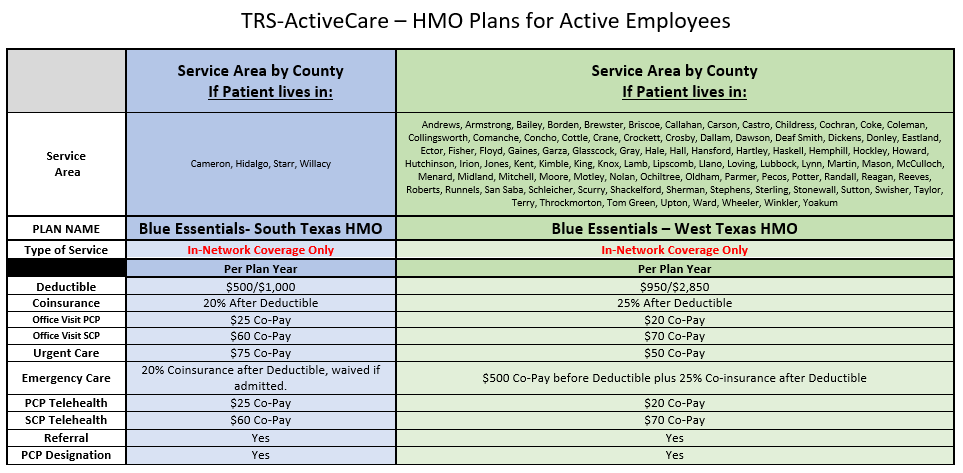
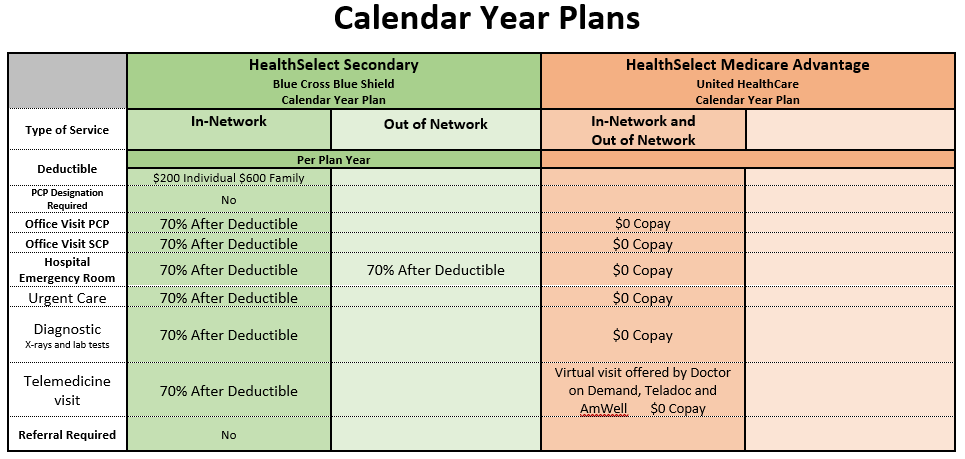
TRS 2025-2026 Plan Year
Products for 2025-2026 Plan Year
Please be aware the Retiree Plans are Calendar Year
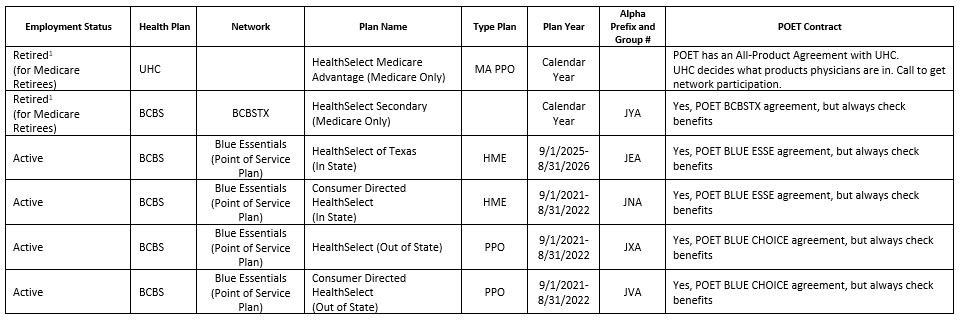
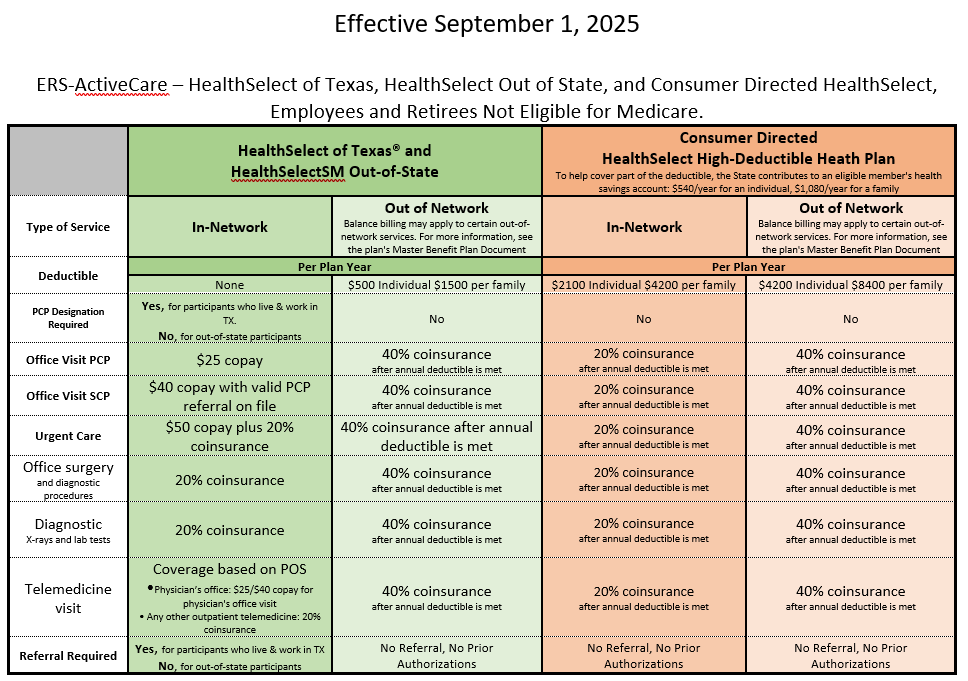
ERS 2025-2026 Plan Year
Products for 2025-2026 Plan Year
Please be aware the Retiree Plans are Calendar Year
Recent Comments