Tag: CMS (Medicare and Medicaid)
Final 2026 Medicare Conversion Factors: What Providers Need to Know
Understanding the difference between QP and non-QP conversion factors
Each year, the Centers for Medicare & Medicaid Services (CMS) finalizes updates that impact Medicare reimbursement under the Physician Fee Schedule (PFS). One of the most important updates is the Medicare Conversion Factor (CF) — the dollar amount used to convert Relative Value Units (RVUs) into the final payment amount.
For Calendar Year (CY) 2026, CMS finalized two separate conversion factors:
One for Qualifying Participants (QPs) in Advanced Alternative Payment Models (Advanced APMs)
One for Non-Qualifying Participants (Non-QPs)
This distinction is important because it directly affects reimbursement rates depending on a provider’s participation status in the Quality Payment Program (QPP).
Qualifying Participants (QPs)
A provider becomes a QP by meeting specific thresholds for participation in Advanced APMs, such as having a certain percentage of payments or patients through eligible Advanced APM arrangements.
Key point: QPs receive a more favorable conversion factor update than non-QPs.
Non-Qualifying Participants (Non-QPs)
Providers who do not meet QP thresholds—or who participate in MIPS instead—fall into the non-QP category.
Bottom Line:
The Final 2026 Medicare Conversion Factors reinforce a major policy direction: CMS continues to differentiate payment updates based on participation in Advanced APMs.
Understanding whether your clinicians are QPs or non-QPs is essential for accurate reimbursement forecasting and strategic planning.
Conversion Factor:
- $33.57 for qualifying alternative payment model (APM) participants (QPs)
- $33.40 for non-QPs
- An increase of 3.77% for QPs and 3.26% for non-QPs over the 2025 rates
- Includes 0.75% increase for QPs and 0.25 for non-QPs
- 0.49% positive budget neutrality adjustment
- 2.50% increase from the OBBBA for 2026
HealthSpring Provider Manual 2026
Have you received your copy of the HealthSpring Provider Manual?
The Definition of G0136 is Changing
Another Great Article from CodingIntel
November 2025
|
Medicare Beneficiaries Involved in CMS Data Breach
CMS Notifies Individuals Potentially Impacted by Data Incident
Approximately 103,000 beneficiaries may have been impacted.
POET has been told by several offices, they are seeing beneficiaries who have been assigned a new number by CMS.
CMS Instructs MACs to Lift Claims Hold

Special edition – courtesy of Novitas Solutions
Claims Hold Update
CMS instructed all Medicare Administrative Contractors (MACs) to lift the claims hold and process claims with dates of service of October 1, 2025, and later for certain services impacted by select expired Medicare legislative payment provisions passed under the Full-Year Continuing Appropriations and Extensions Act, 2025 (Pub. L. 119-4, Mar. 15, 2025). This includes claims paid under the Medicare Physician Fee Schedule, ground ambulance transport claims, and Federally Qualified Health Center (FQHC) claims. This includes telehealth claims that CMS can confirm are definitively for behavioral and mental health services. CMS has directed all MACs to continue to temporarily hold claims for other telehealth services (i.e. those that CMS cannot confirm are definitively for behavioral and mental health services) and for acute Hospital Care at Home claims.
Beginning October 1, 2025, for services that are not behavioral health services, many of the statutory limitations on payment for Medicare telehealth services that were, in response to the COVID-19 Public Health Emergency, lifted, and subsequently extended, through legislation again took effect. These include prohibition of many services provided to beneficiaries in their homes and outside of rural areas, and hospice recertifications that require a face-to-face encounter. In the absence of Congressional action, practitioners who choose to perform telehealth services that are not payable by Medicare on or after October 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage (ABN). Further information on use of the ABN, including ABN forms and form instructions: https://www.cms.gov/medicare/forms-notices/beneficiary-notices-initiative/ffs-abn. Practitioners should monitor Congressional action and may choose to hold claims associated with telehealth services that are currently not payable by Medicare in the absence of Congressional action. For further information: https://www.cms.gov/medicare/coverage/telehealth.
CMS notes that the Bipartisan Budget Act of 2018 (Pub. L. 115-123, Feb. 9, 2018), which added section 1899(l) to the Social Security Act, allows clinicians in applicable Medicare Shared Savings Program Accountable Care Organizations (ACOs) to provide and receive payment for covered telehealth services to certain Medicare beneficiaries without geographic restrictions and in the beneficiary’s home. Separate from requirements to participate in the Medicare Shared Savings Program, there is no special application or approval process for applicable ACOs or their ACO participants or ACO providers/suppliers to offer these covered telehealth services. Clinicians in applicable ACOs can furnish and receive payment for covered telehealth services under these special telehealth flexibilities. For clinicians in applicable ACOs, telehealth claims that CMS can confirm are definitively for behavioral and mental health services will be paid. At this time, claims for some telehealth services will continue to be held. For more information, including information on to which ACOs these flexibilities apply: https://www.cms.gov/files/document/shared-savings-program-telehealth-fact-sheet.pdf.
Goverment Shutdown: What you Need to Know
With the government shutdown in effect, the Texas Medical Association is in regular communication with federal colleagues at the American Medical Association on the impact to physician practices, as AMA remains in touch with senior officials at the Centers for Medicare & Medicaid Services (CMS).
The volatility in Washington, D.C. could mean the shutdown lasts days to weeks, and TMA will share additional information via Texas Medicine Today as the situation develops. Here is what physicians need to know so far:
Medicare/Medicaid: The CMS contingency plan states that during a lapse in funding, the Medicare program will continue. CMS also says it has sufficient funding for Medicaid to fund the first quarter of 2026 and is maintaining the staff necessary to make payments to eligible states for the Children’s Health Insurance Program.
Medicare Administrative Contractors (MACs) have been instructed to implement a temporary claims hold of 10 business days, which AMA says should have minimal impact on physicians due to the 14-day payment floor. “The hold prevents the need for reprocessing large volumes of claims should Congress act after the statutory expiration date,” states a CMS Medicare Learning Network Connects special edition email newsletter that, as of this writing, had not yet been publicly posted. Physicians may continue to submit claims during this period, but payment will not be released until the hold is lifted. For the latest information, AMA recommends physicians monitor their MAC’s website (Novitas in Texas) and this CMS webpage.
“In the past, Congress generally has restored lapsed policies back to the effective date of the shutdown. During the shutdown, the AMA is monitoring any potential delays in Medicare claims processing or other Medicare payment problems that could result from federal staffing reductions at CMS, including during the shutdown,” said AMA CEO and Executive Vice President John Whyte, MD, MPH.
Telehealth: Physicians who provide telehealth services to fee-for-service Medicare patients should be aware that the Medicare telehealth flexibilities lapsed on Sept. 30 for most care and congressional action is required to restore that waiver. The exceptions are patients being treated for mental health and/or behavioral health disorder (including substance use disorders), stroke, and monthly end-stage renal disease visits for home dialysis. Otherwise, telehealth services are limited to rural areas as they were before the COVID public health emergency, and patients cannot receive telehealth services in their homes. The ability to provide audio-only services to Medicare patients also lapsed, as did the Acute Hospital Care at Home program.
The CMS newsletter suggests “practitioners who choose to perform telehealth services that are not payable by Medicare on or after Oct. 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage.”
However, AMA notes physicians in certain Medicare Shared Savings Program accountable care organizations can continue to provide and be paid for telehealth services.
Other services: CMS says it is continuing federal insurance marketplace activities, such as eligibility verification. Other nondiscretionary activities including health care fraud and abuse control and Center for Medicare & Medicaid Innovation activities are also continuing.
However, AMA reports that funding extensions for community health centers, the National Health Service Corps, and teaching health centers that operate graduate medical education programs expired on Sept. 30, and the 1.0 work geographic practice cost index floor extension expired on Oct. 1. Additional programs that have lapsed include: special diabetes programs; public health emergency authorities (e.g., Public Health Emergency Fund); increased inpatient hospital payment adjustment for certain low-volume hospitals; the Medicare-Dependent Hospital program; quality measure endorsement, input, and selection; and outreach and assistance for low-income programs (e.g., area agencies on aging).
TMA wants to hear from you. If you or your practice staff experience Medicare payment delays, telehealth obstacles, or other concerns, please let us know through TMA’s Knowledge Center to help inform advocacy.
Amy Lynn Sorrel
Associate Vice President, Editorial Strategy & Programming
Division of Communications and Marketing
CMS Releases 2024 MIPS Scores

The Centers for Medicare & Medicaid Services (CMS) has released MIPS performance feedback and final scores for the 2024 performance year. Sign in to the Quality Payment Program (QPP) website using your Health Care Quality Information Systems (HCQIS) Access Roles and Profile (HARP) system credentials to view your feedback from CMS. The targeted review period will be open for approximately 60 days, beginning with the release of final scores and closing 30 days after the release of MIPS payment adjustments that CMS plans to announce in one month.
VA Seeking Refunds for Past CHAMPVA Claims
The U.S. Department of Veterans Affairs (VA) announced it aims to recover more than $41 million in “overpaid claims” paid to physicians and other health care professionals and entities through the Civilian Health and Medical Program of the Department of Veterans Affairs (CHAMPVA) program.
Texas Medical Association staff caution that physicians receiving CHAMPVA refund requests should take several steps to satisfy the VA request without immediately losing payment for care already delivered:
- Confirm the legitimacy of the request letter. As refund letters typically come from third-party companies, a practice may call CHAMPVA and ask them if the third-party company is one they contracted with to collect the overpayment;
- Check the letter for details on how to appeal, including any payment or appeal deadlines; and
- Check the letter for information about which insurer VA says is responsible for payment.
From there, physicians can choose one of two actions. If it appears the alleged overpayment has been identified in error, start the appeal process to try to keep the CHAMPVA payment already received. If not pursuing an appeal – or if an appeal is ultimately denied – refund the overpayment to VA and seek payment from the insurer VA says is responsible for payment. For a physician seeking payment from that insurer, TMA recommends including, as part of that request, the initial CHAMPVA explanation of benefits and any information from VA indicating that the insurer is the proper payer, especially if the filing deadline has passed.
For assistance with CHAMPVA refund requests or other payment matters, contact TMA’s Physician Payment Resource Center.
Separate Services, Same Date of Service
With health plans increasingly adopting payment protocols that hinder physicians from providing multiple services on the same day – despite previously covering such services – delegates adopted policy calling on TMA to “advocate for legislation or regulation that would prevent Medicaid and commercial payers from denying payment for distinct, separate services provided on the same day.”
Delegates agreed with physicians’ concerns that these payer practices often force patients to forego care.
“This especially hurts patients who either have to travel long distances to see their physician or have transportation issues that prevent them from making multiple trips,” Odessa allergist and immunologist Vivek Rao, MD, wrote in online testimony on behalf of the Lone Star Caucus
Other measures adopted by the house to eliminate payment-related barriers to patient care direct TMA to pursue state-level legislation or regulation that:
- Prohibits insurers, plan sponsors, third party administrators, and other contracted identities from recouping previously paid claims due to retroactive termination of patient coverage;
- Imposes payer communication standards – with penalties – that provide patients, physicians, and others with timely access to a live representative; and
- Expedites prior authorization approvals for hospice care in emergency and acute care settings, eliminates deductibles for hospice care, and provides clear disclosures detailing hospice care benefits in policy documents as well as online.
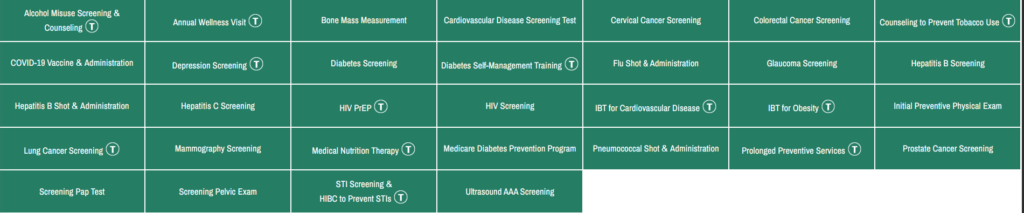
Medicare Preventive Services – Revised
The above link will lead you to MLN Educational Tool, where you can click a service and see the changes.
Recent Comments