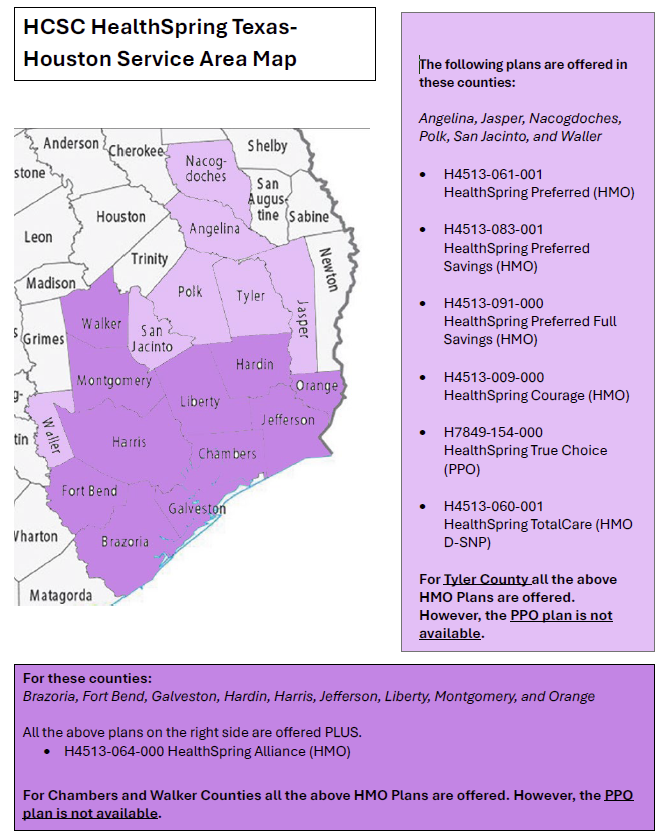
POET staff has done everything short of a full skeletal reconstruction to make the HealthSpring county page in the provider manual legible. They’ve stretched it. They’ve shrunk it. They’ve even converted it to Word and back to a PNG. It just didn’t have the backbone it needed.
If we were tibia honest, nothing worked.
So I, Sir Seymore Bones — resident WordPress writer and part-time osteo-optimizer — took pen in hand (metacarpals and all) to give everyone a little relief. When the formatting started rattling, I decided it was time to get to the bare bones of the issue.
I hope the map below helps you Sey-more, and make sense of the plans offered in our counties. We femur-ly believe this version is better. If it doesn’t… well, I promise I didn’t bone it up on purpose.
Understanding the difference between QP and non-QP conversion factors
Each year, the Centers for Medicare & Medicaid Services (CMS) finalizes updates that impact Medicare reimbursement under the Physician Fee Schedule (PFS). One of the most important updates is the Medicare Conversion Factor (CF) — the dollar amount used to convert Relative Value Units (RVUs) into the final payment amount.
For Calendar Year (CY) 2026, CMS finalized two separate conversion factors:
One for Qualifying Participants (QPs) in Advanced Alternative Payment Models (Advanced APMs)
One for Non-Qualifying Participants (Non-QPs)
This distinction is important because it directly affects reimbursement rates depending on a provider’s participation status in the Quality Payment Program (QPP).
Qualifying Participants (QPs)
A provider becomes a QP by meeting specific thresholds for participation in Advanced APMs, such as having a certain percentage of payments or patients through eligible Advanced APM arrangements.
Key point: QPs receive a more favorable conversion factor update than non-QPs.
Non-Qualifying Participants (Non-QPs)
Providers who do not meet QP thresholds—or who participate in MIPS instead—fall into the non-QP category.
Bottom Line:
The Final 2026 Medicare Conversion Factors reinforce a major policy direction: CMS continues to differentiate payment updates based on participation in Advanced APMs.
Understanding whether your clinicians are QPs or non-QPs is essential for accurate reimbursement forecasting and strategic planning.
Conversion Factor:
$33.57 for qualifying alternative payment model (APM) participants (QPs)
$33.40 for non-QPs
An increase of 3.77% for QPs and 3.26% for non-QPs over the 2025 rates
Includes 0.75% increase for QPs and 0.25 for non-QPs
0.49% positive budget neutrality adjustment
2.50% increase from the OBBBA for 2026
MAKE SURE YOU ARE PULLING THE CORRECT FEE SCHEDULE FOR YOUR PRACTICE
POET understands, not everyone is a biller, and we might be throwing out alphabet soup to some office personal.
What is a CMS-1500 (HCFA) Form?
The CMS-1500, often still called a HCFA, is the standard paper form used to bill insurance companies for professional services provided by physicians and other healthcare providers.
It tells the insurance company:
Who the patient is
Who the provider is
What services were performed
When the services occurred
Why they were medically necessary
How much is being charged
What is Used When Claims Are Filed Electronically?
When an office files claims electronically, the equivalent of the CMS-1500 form is an: ANSI 837P Claim
837 = electronic claim format
P = Professional services
The 837P contains the same information as a CMS-1500, just in a computer-readable format instead of paper.
Why Staff May Not “See” an 837P
The billing software creates it automatically
It is sent through a clearinghouse
Insurance companies process it behind the scenes
Most staff interact with screens and reports, not the actual electronic file.
If You Need to See a “Paper Copy” of an 837P
An 837P does not have a true paper form. However, billing systems can produce a claim print image or CMS-1500-style report that shows the same data contained in the electronic claim.
This is often called:
Claim print image
CMS-1500 claim view
Electronic claim summary
These reports are used for: (Why POET would request it)
Reviewing what was sent
Troubleshooting rejections or denials
Sharing claim details with non-billing staff
Important: This is a readable representation of the 837P data — not the actual electronic file.
To see the raw 837P file itself, billing staff would need to export or view it through the billing system or clearinghouse.
Disclaimer: The information provided in this blog is for general educational purposes only. While Ink strives to explain insurance concepts accurately and clearly, payer rules, contracts, and policies can vary widely by plan, state, and provider agreement—and they change frequently.
This content should not be interpreted as definitive guidance or a substitute for reviewing payer manuals, contracts, or official communications. Physician offices are encouraged to conduct their own research and verify requirements directly with the applicable insurance carriers before making operational or billing decisions.
🎯 ERISA Plan vs. Third-Party Administrator (TPA) They’re not the same thing — and mixing them up causes a LOT of confusion.
🌈 Think of it like this:
🏛️ ERISA Plan = The Rulebook
This is the actual health plan created by the employer.
It spells out:
✔️ What’s covered ✔️ What’s excluded ✔️ How claims should be paid ✔️ Who has final authority
📌 The employer owns the ERISA plan and carries the responsibility.
⚙️ Third-Party Administrator (TPA) = The Referee
They simply:
✔️ Process claims ✔️ Apply the plan rules ✔️ Handle paperwork & customer service
📌 The TPA follows the rules — they don’t make them
💡 Why this matters: 👉 An ERISA plan can change TPAs 👉 A TPA cannot change the ERISA plan 👉 Coverage decisions come from the plan document, not the administrator
✨ Bottom line: 🧠 ERISA Plan = The Authority 🛠️ TPA = The Administrator
Understanding the difference protects employers, providers, and members alike.
Disclaimer: The information provided in this blog is for general educational purposes only. While Ink strives to explain insurance concepts accurately and clearly, payer rules, contracts, and policies can vary widely by plan, state, and provider agreement—and they change frequently.
This content should not be interpreted as definitive guidance or a substitute for reviewing payer manuals, contracts, or official communications. Physician offices are encouraged to conduct their own research and verify requirements directly with the applicable insurance carriers before making operational or billing decisions
BCBSTX has notified POET that a NEW Fee Schedule for Blue Choice and Blue Essentials will be effective May 1, 2026.
Once POET receives the new fee schedule and completes its review, OPT-IN / OPT-OUT packets will be sent to physician offices for participation decisions.
Please watch for additional communication once the review process is complete

Recent Comments