Tag: Telehealth
CMS Instructs MACs to Lift Claims Hold

Special edition – courtesy of Novitas Solutions
Claims Hold Update
CMS instructed all Medicare Administrative Contractors (MACs) to lift the claims hold and process claims with dates of service of October 1, 2025, and later for certain services impacted by select expired Medicare legislative payment provisions passed under the Full-Year Continuing Appropriations and Extensions Act, 2025 (Pub. L. 119-4, Mar. 15, 2025). This includes claims paid under the Medicare Physician Fee Schedule, ground ambulance transport claims, and Federally Qualified Health Center (FQHC) claims. This includes telehealth claims that CMS can confirm are definitively for behavioral and mental health services. CMS has directed all MACs to continue to temporarily hold claims for other telehealth services (i.e. those that CMS cannot confirm are definitively for behavioral and mental health services) and for acute Hospital Care at Home claims.
Beginning October 1, 2025, for services that are not behavioral health services, many of the statutory limitations on payment for Medicare telehealth services that were, in response to the COVID-19 Public Health Emergency, lifted, and subsequently extended, through legislation again took effect. These include prohibition of many services provided to beneficiaries in their homes and outside of rural areas, and hospice recertifications that require a face-to-face encounter. In the absence of Congressional action, practitioners who choose to perform telehealth services that are not payable by Medicare on or after October 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage (ABN). Further information on use of the ABN, including ABN forms and form instructions: https://www.cms.gov/medicare/forms-notices/beneficiary-notices-initiative/ffs-abn. Practitioners should monitor Congressional action and may choose to hold claims associated with telehealth services that are currently not payable by Medicare in the absence of Congressional action. For further information: https://www.cms.gov/medicare/coverage/telehealth.
CMS notes that the Bipartisan Budget Act of 2018 (Pub. L. 115-123, Feb. 9, 2018), which added section 1899(l) to the Social Security Act, allows clinicians in applicable Medicare Shared Savings Program Accountable Care Organizations (ACOs) to provide and receive payment for covered telehealth services to certain Medicare beneficiaries without geographic restrictions and in the beneficiary’s home. Separate from requirements to participate in the Medicare Shared Savings Program, there is no special application or approval process for applicable ACOs or their ACO participants or ACO providers/suppliers to offer these covered telehealth services. Clinicians in applicable ACOs can furnish and receive payment for covered telehealth services under these special telehealth flexibilities. For clinicians in applicable ACOs, telehealth claims that CMS can confirm are definitively for behavioral and mental health services will be paid. At this time, claims for some telehealth services will continue to be held. For more information, including information on to which ACOs these flexibilities apply: https://www.cms.gov/files/document/shared-savings-program-telehealth-fact-sheet.pdf.
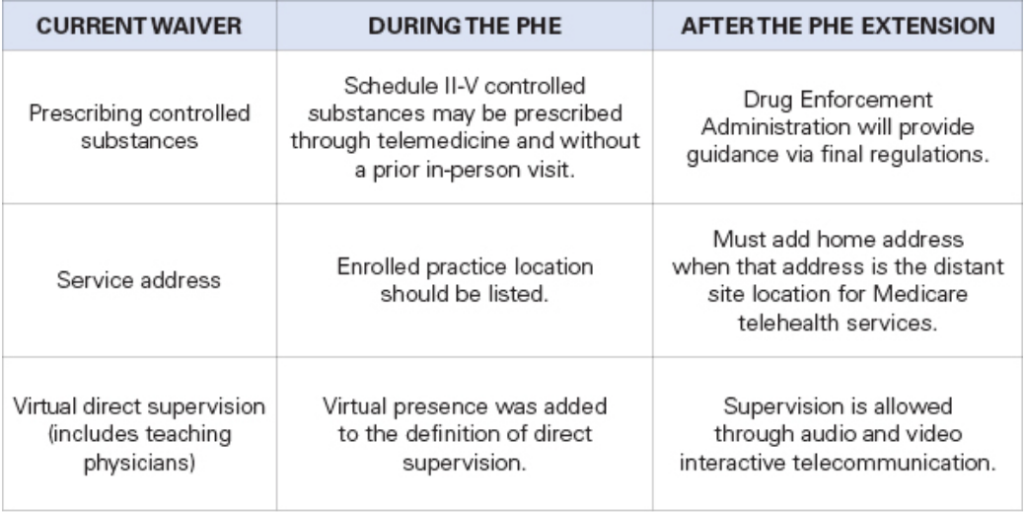
More Telehealth Waivers Set to Expire Dec. 31
As TMA monitors the government shutdown and the coinciding expiration of certain telehealth waivers as of Sept. 30, physicians should take notice of another series of telehealth waivers set to expire at the end of this year.
TMA staff note that Medicare Advantage plans don’t have to follow Medicare’s policy on the waiver expirations.
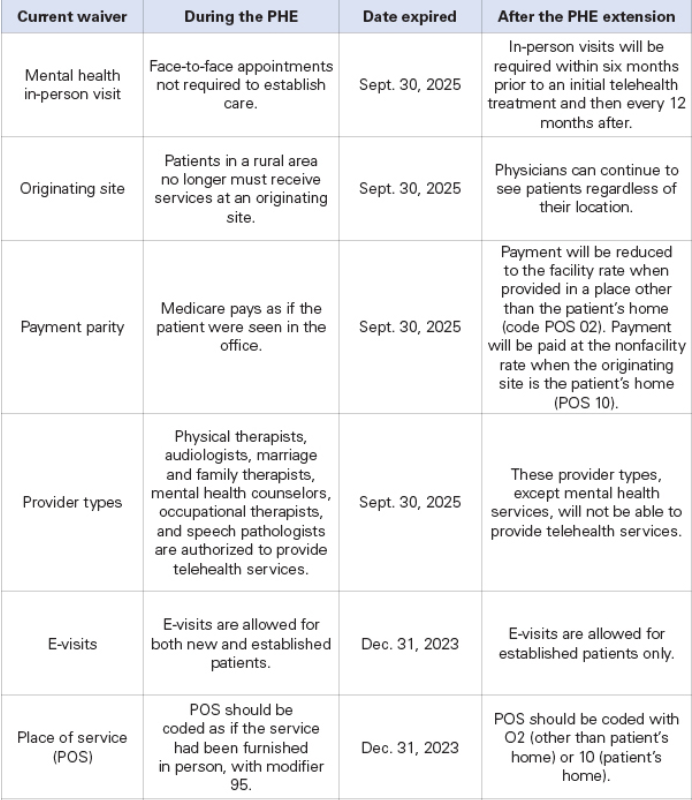
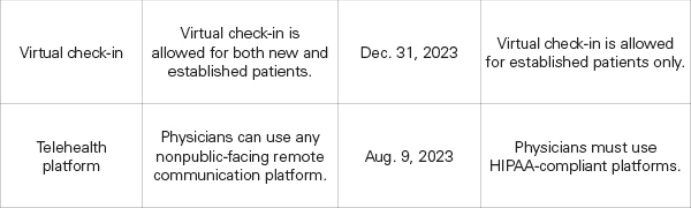
The following waivers enacted during the COVID-19 public health emergency (PHE) are currently expected to expire Dec. 31 unless Congress acts:
The following waivers have already expired:
Goverment Shutdown: What you Need to Know
With the government shutdown in effect, the Texas Medical Association is in regular communication with federal colleagues at the American Medical Association on the impact to physician practices, as AMA remains in touch with senior officials at the Centers for Medicare & Medicaid Services (CMS).
The volatility in Washington, D.C. could mean the shutdown lasts days to weeks, and TMA will share additional information via Texas Medicine Today as the situation develops. Here is what physicians need to know so far:
Medicare/Medicaid: The CMS contingency plan states that during a lapse in funding, the Medicare program will continue. CMS also says it has sufficient funding for Medicaid to fund the first quarter of 2026 and is maintaining the staff necessary to make payments to eligible states for the Children’s Health Insurance Program.
Medicare Administrative Contractors (MACs) have been instructed to implement a temporary claims hold of 10 business days, which AMA says should have minimal impact on physicians due to the 14-day payment floor. “The hold prevents the need for reprocessing large volumes of claims should Congress act after the statutory expiration date,” states a CMS Medicare Learning Network Connects special edition email newsletter that, as of this writing, had not yet been publicly posted. Physicians may continue to submit claims during this period, but payment will not be released until the hold is lifted. For the latest information, AMA recommends physicians monitor their MAC’s website (Novitas in Texas) and this CMS webpage.
“In the past, Congress generally has restored lapsed policies back to the effective date of the shutdown. During the shutdown, the AMA is monitoring any potential delays in Medicare claims processing or other Medicare payment problems that could result from federal staffing reductions at CMS, including during the shutdown,” said AMA CEO and Executive Vice President John Whyte, MD, MPH.
Telehealth: Physicians who provide telehealth services to fee-for-service Medicare patients should be aware that the Medicare telehealth flexibilities lapsed on Sept. 30 for most care and congressional action is required to restore that waiver. The exceptions are patients being treated for mental health and/or behavioral health disorder (including substance use disorders), stroke, and monthly end-stage renal disease visits for home dialysis. Otherwise, telehealth services are limited to rural areas as they were before the COVID public health emergency, and patients cannot receive telehealth services in their homes. The ability to provide audio-only services to Medicare patients also lapsed, as did the Acute Hospital Care at Home program.
The CMS newsletter suggests “practitioners who choose to perform telehealth services that are not payable by Medicare on or after Oct. 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage.”
However, AMA notes physicians in certain Medicare Shared Savings Program accountable care organizations can continue to provide and be paid for telehealth services.
Other services: CMS says it is continuing federal insurance marketplace activities, such as eligibility verification. Other nondiscretionary activities including health care fraud and abuse control and Center for Medicare & Medicaid Innovation activities are also continuing.
However, AMA reports that funding extensions for community health centers, the National Health Service Corps, and teaching health centers that operate graduate medical education programs expired on Sept. 30, and the 1.0 work geographic practice cost index floor extension expired on Oct. 1. Additional programs that have lapsed include: special diabetes programs; public health emergency authorities (e.g., Public Health Emergency Fund); increased inpatient hospital payment adjustment for certain low-volume hospitals; the Medicare-Dependent Hospital program; quality measure endorsement, input, and selection; and outreach and assistance for low-income programs (e.g., area agencies on aging).
TMA wants to hear from you. If you or your practice staff experience Medicare payment delays, telehealth obstacles, or other concerns, please let us know through TMA’s Knowledge Center to help inform advocacy.
Amy Lynn Sorrel
Associate Vice President, Editorial Strategy & Programming
Division of Communications and Marketing
Government Shutdown Changes

What has changed due to the Government Shutdown?
It’s pandemic-era flexibilities that will come to an end:
- Geographic restrictions that only permitted telehealth in medically underserved areas
- Requiring the patient to go to an originating site (a health care facility) instead of being in their homes
- Allowing therapists (PTs, OTs, SLPS, audiologists) to perform services via telehealth
Behavioral health via telehealth will still be allowed after September 30th, because Congress passed a law allowing it permanently. It won’t be affected by a government shutdown, if one occurs. The Social Security Act references “mental health” as opposed to “behavioral”.
Quoting the MLN Matters Article on E/M services
MLN006764 September 2025
Telehealth Services
Section 2207 of the Full-Year Continuing Appropriations and Extensions Act, 2025, extended many of these flexibilities through September 30th, 2025. Starting October 1, 2025, the statutory limitations that were in place for Medicare telehealth services before the COVID-19 public health emergency (PHE) will retake effect for most telehealth services.
These include:
- Geographic restrictions
- Location restrictions on where you can provide services
- Limitations on the scope of practitioners who can provide telehealth services
That is, telehealth as we know it to anywhere in the country, in the patient’s home ends. How do you know if you are in an underserved area, and can continue to do telehealth? Quick and easy: could your practice do telehealth before the pandemic? Yes: in all likelihood, you can continue, but remember the patient must go to an originating site, not their homes. Are you in an underserved area? Check here.
At CodingIntel, we have a copy of the CMS telehealth fact sheet from prior to the pandemic. It isn’t up-to-date with the list below, but it will tell you the rules for most practices in the country if a shutdown occurs.
Still allowed are services that weren’t implemented as a result of the pandemic.
eCFR :: 42 CFR 410.78 — Telehealth services.
(iv) The geographic requirements specified in paragraph (b)(4) of this section do not apply to the following telehealth services:
(A) Home dialysis monthly ESRD-related clinical assessment services furnished on or after January 1st, 2019, at an originating site described in paragraphs (b)(3)(vi), (ix), or (x) of this section, in accordance with section 1881(b)(3)(B) of the Act; and
(B) Services furnished on or after January 1st, 2019, for purposes of diagnosis, evaluation, or treatment of symptoms of an acute stroke.
(C) Services furnished on or after July 1st, 2019, to an individual with a substance use disorder diagnosis, for purposes of treatment of a substance use disorder or a co-occurring mental health disorder.
(D) Services furnished on or after January 1st, 2025, for the purposes of diagnosis, evaluation, and/or treatment of a mental health disorder. Payment will not be made for a telehealth service furnished under this paragraph unless the physician or practitioner has furnished an item or service in person, without the use of telehealth, for which Medicare payment was made (or would have been made if the patient were entitled to, or enrolled for, Medicare benefits at the time the item or service is furnished) within 6 months prior to the initial telehealth service and within 6 months of any subsequent telehealth service.
Betsy
CMS Telehealth FAQ Calendar Year 2025
Q1: Do Medicare beneficiaries need to be located in a rural area and in a medical facility in order to receive Medicare telehealth services?
A1: Pursuant to the American Relief Act, 2025, beneficiaries can continue to receive Medicare telehealth services wherever in the United States and territories they’re located, including in their home, through March 31, 2025. They don’t need to be in a rural area or a medical facility.
Q2: Are there any restrictions on the types of practitioners who can furnish Medicare telehealth services?
A2: Pursuant to the American Relief Act, 2025, through March 31, 2025, any practitioner who can independently bill Medicare for their professional services may furnish telehealth. This includes physical therapists, occupational therapists, speech-language pathologists, and audiologists.
Q3: Can outpatient therapy, diabetes self-management training and medical nutrition therapy services be furnished remotely by hospital staff to beneficiaries in their homes ?
A3: As we explained in the CY 2025 OPPS/ASC final rule with comment period, we have generally aligned payment policies for outpatient therapy services, diabetes self-management training (DSMT) and medical nutrition therapy (MNT) services furnished remotely by hospital staff to beneficiaries in their homes with policies for Medicare telehealth services. We noted in the CY 2025 OPPS/ASC proposed rule that, to the extent therapists and DSMT and MNT practitioners continue to be distant site practitioners for purposes of Medicare telehealth services, we anticipated aligning our policy for these services with policies under the Physician Fee Schedule (PFS) and continuing to make payment to the hospital for these services when furnished by hospital staff. When the CY 2025 OPPS/ASC final rule was issued, the flexibility to allow an expanded range of practitioners to be eligible to furnish Medicare telehealth services, which included physical therapists (PTs), occupational therapists (OTs), and speech language pathologists (SLPs), was set to expire at the end of CY 2024. Consequently we stated that we would no longer pay for outpatient therapy, DSMT, and MNT services when furnished remotely by hospital staff to beneficiaries in their homes beginning in CY 2025, but we also noted that continuing to align our policies for outpatient therapy, DSMT, and MNT services when furnished by hospital staff with the Medicare telehealth policies that apply when these services are billed by the same clinicians but in private practice ensures clarity and consistency for providers and beneficiaries.
The American Relief Act, 2025 extended the expansion of the types of practitioners eligible to furnish Medicare telehealth services through March 31, 2025, thus enabling PTs, OTs, and SLPs to continue furnishing telehealth services through that date. CMS is continuing to align our requirements for payment for services furnished remotely by hospital staff to beneficiaries in their homes, including remotely furnished outpatient therapy services, DSMT, and MNT services, with requirements for Medicare telehealth services. Therefore, through March 31, 2025, hospitals can continue to bill for these services when furnished remotely by hospital staff to beneficiaries in their homes.
Q4: How does CMS make payment for telehealth services furnished in RHCs and FQHCs? Can Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs) continue to serve as distant sites for the provision of telehealth services?
A4: Any behavioral health service furnished by an RHC or FQHC on or after January 1, 2022 through interactive telecommunications technology is paid under the All Inclusive Rate (AIR) and Prospective Payment System (PPS), respectively. Through March 31, 2025, RHCs and FQHCs may continue to bill for non-behavioral health services furnished through interactive telecommunications technology by reporting HCPCS code G2025 on the claim.
Q5: Will in person visit requirements apply to behavioral health services furnished by professionals through Medicare telehealth? What about behavioral health services furnished remotely by hospital staff to beneficiaries in their homes, or behavioral health visits furnished by RHCs, and FQHCs where the patient is present virtually?
A5: The American Relief Act, 2025 has delayed in-person visit requirements for behavioral health services for professionals billing for Medicare telehealth services until April 1, 2025.
Regarding behavioral health services furnished remotely by hospital staff to beneficiaries in their homes, we are continuing to align our policy with requirements for Medicare telehealth services billed under the PFS. Accordingly, we are also delaying the in-person visit requirements for these services until April 1, 2025.
In the CY 2025 PFS final rule, we finalized that for behavioral health visits furnished by RHCs and FQHCs where the patient is present virtually, we are delaying in-person visit requirements until January 1, 2026.
Q6: Can beneficiaries continue to receive audio-only telehealth services? Are audio-only telehealth services permitted in all originating sites?
A6: Pursuant to the American Relief Act, 2025, physicians and practitioners may continue to use two-way, real-time audio-only communication technology for Medicare telehealth services furnished through March 31, 2025.
After March 31, 2025, physicians and practitioners may continue to use two-way, real-time audio-only communication technology to furnish Medicare telehealth services in accordance with the revised definition of “interactive telecommunications system”. In the CY 2025 PFS final rule, CMS permanently changed the definition of “interactive telecommunications system” to include two-way, real-time audio-only communication technology for any telehealth service furnished to a patient in their home, provided that the furnishing physician or practitioner is technically capable of using audio-video communication technology and that the beneficiary is not capable of or does not consent to using audio-video communication technology. Audio-only can be used for both new and established patients. Beneficiaries who are receiving remote mental health services, as defined in the CY 2023 and 2024 OPPS Final Rules, furnished by hospital-employed staff in their homes may permanently receive these via audio-only communication technology.
Pursuant to the American Relief Act, 2025, audio-only telehealth services are permitted in all originating sites through March 31, 2025. However, in general, audio-only telehealth services are only permitted if the beneficiary is in their home. All other originating sites are medical facilities that generally have the infrastructure and broadband capacity to support two-way, audio/video communication technology. Additionally, patients would not have the same heightened expectation of privacy when video is used for a Medicare telehealth service in a medical facility as they would in their home.
Q7: What are the current guidelines for virtual presence for teaching physicians who furnish telehealth services involving residents?
A7: In the CY 2025 PFS final rule, we established that through December 31, 2025, we are continuing to allow teaching physicians to have a virtual presence in all teaching settings, but only for services furnished as a Medicare telehealth service. This will continue to permit teaching physicians to have a virtual presence during the key portion of the Medicare telehealth service for which payment is sought, through audio/video real-time communications technology, for all residency training locations through December 31, 2025.
Q8: Which place of service code should I use for telehealth services?
A8: Physicians and/or practitioners should use POS 02 for Telehealth Provided Other than in Patient’s Home or POS 10 for Telehealth Provided in Patient’s Home (which is a location other than a hospital or other facility where the patient receives care in a private residence). In the CY 2024 PFS final rule, we finalized that, starting January 1, 2024, claims for Medicare telehealth services provided to patients in their homes are to be paid at the non-facility payment rate.
Q9: Are there frequency limitations for subsequent inpatient and nursing facility visits and critical care consultations?
A9: In the CY 2025 PFS final rule, we established that through December 31, 2025, we are continuing to suspend the application of telehealth frequency limits on subsequent inpatient and nursing facility visits and critical care consultations.
Q10: Which services allow virtual direct supervision?
A10: For all services requiring direct supervision, we continue to permit direct supervision to be provided through real-time audio/video only through December 31, 2025. This applies to all services where direct supervision is required, including most incident-to services under § 410.26, many diagnostic tests under § 410.32, pulmonary rehabilitation services under § 410.47, cardiac rehabilitation and intensive cardiac rehabilitation services under § 410.49, and certain hospital outpatient services as provided under § 410.27(a)(1)(iv).In the CY 2025 PFS final rule, we finalized that for a certain subset of services valued under the PFS that are typically performed in their entirety by auxiliary personnel that are required to be furnished under direct supervision, we permanently adopted a definition of direct supervision that allows virtual presence through real-time audio and video communications technology.
Q11: Are there geographic or place of service restrictions for behavioral health telehealth services (including SUD services)?
A11: No. The Consolidated Appropriations Act, 2021 permanently removed geographic and place of service restrictions for behavioral health telehealth services. Beneficiaries, including those in both rural and urban areas, can receive behavioral health telehealth services in their homes. Two-way, interactive, audio-only technology is permitted for behavioral health telehealth services.
Q12: What does the “provisional” or “permanent” designation mean on the Medicare Telehealth Services List?
A12: In the CY 2024 PFS final rule (88 FR 78861 through 78866), we implemented a revised 5-step process for making additions, deletions, and changes to the Medicare Telehealth Services List (5-step process), beginning for the CY 2025 Medicare Telehealth Services List. Rather than categorizing a service as “Category 1” or “Category 2,” each service is now assigned a “permanent” or “provisional” status. A service is assigned a “provisional” status if available evidence does not yet demonstrate that the service is definitively of clinical benefit, but there is enough evidence to suggest that further study may demonstrate such benefit. The 5-step process review criteria are set forth in the CY 2024 PFS final rule (88 FR 78861 through 78866) and listed at https://www.cms.gov/medicare/coverage/telehealth/criteria-request.
Q13: Do services with a “provisional” designation expire each calendar year?
A13: No, there is no time limitation for services designated as “provisional” on the Medicare Telehealth Services List . We did not consider for CY 2025 whether to recategorize provisional codes as permanent because we intend to conduct a comprehensive evaluation of all Medicare telehealth services with provisional status. Services included on the Medicare Telehealth Services List with provisional status will remain on the list. We anticipate addressing these services in future rulemaking.
Q14: How do I request a change to the Medicare Telehealth Services List?
A14: Requests for changes to the Medicare Telehealth Services List must be received by CMS by February 10 of a year to be considered by CMS and addressed in PFS rulemaking for the following calendar year. Each request to add a service to the Medicare Telehealth Services List must include any supporting documentation the requester wishes us to consider as we review the request. Because we use the annual PFS rulemaking process to make changes to the Medicare Telehealth Services List, requesters are advised that any information submitted as part of a request is subject to public disclosure for this purpose. For more information on submitting a request to add or modify services on the Medicare Telehealth Services List, including where to send these requests, and to view the current Medicare Telehealth Services List, see our website at https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/index.html.
Q15: Why are non-face-to-face services (such as, but not limited to, Community Health Integration, Principal Illness Navigation, Chronic Care Management, Behavioral Health Integration, and Remote Monitoring) not on the Medicare Telehealth Services List?
A15: For these and similarly situated, non-face-to-face services, the telehealth restrictions are not applicable. Section 1834(m) of the Act limits payment for Medicare telehealth services to services that are in whole or in part, an inherently face-to-face service. Only services that serve as a substitute for an in-person encounter can be classified as a Medicare telehealth service. Services that do not require the presence of, or involve interaction with, the patient fall outside this definition. As discussed in prior rulemaking cycles, because these services do not serve as a substitute for an in-person encounter, we do not consider them to be Medicare telehealth services.
Telehealth Breaking News

The below information was received today 12/26/2024, from Betsy Nicoletti
Medicare practitioners and patients can continue to perform/receive telehealth services as they have since the start of the pandemic for the next three months.
The first keep-the-government-open bill from Dec. 20 extended Medicare telehealth for two years. It didn’t pass. The bill that passed and was signed into law extends telehealth for Medicare patients as we know it now until March 31, 2025. Then, Congress must ACT again or we have the return to the pre-pandemic rules
Does this mean we can use the new CPT telehealth codes 98000-98015?
NOT FOR MEDICARE PATIENTS
98000-98015 have a status indicator of INVALID
Continue to use office visit codes with POS 02 or POS 10
And Other Payers?
Sadly, each payer can make their own telehealth rules.
Have Questions About Capturing Telehealth Visits?
Teleheath appears to become increasingly complex on a daily basis.
The following is a list of guidelines provided by MGMA:
Click on the title to follow the link.
Good News, Bad News in Medicare 2025
A first look at the 2025 Physician Fee Schedule
The 2025 Physician Fee Schedule proposed rule is a study in contrasts. If you’re the kind of person who can see both sides of an issue, this rule is for you.
Good News
Bad News
Practitioners doing telehealth from their home can continue to use the practice address instead of their home address on claims for 2025
Without an act of Congress, for real time audio/visual visits on 1/1/2025 patients can no longer receive these services in their homes in all geographic areas. Patients must be in an underserved area and go to a facility setting for telehealth. (Unless Congress changes this in their end of year Consolidated Appropriations Act.)
16 new telehealth codes that can be selected based on Medical Decision Making (MDM) or time.
Medicare has given them a status indicator of invalid.
New HCPCS code for GIDXX for visit complexity inherent to in patient and observation services associated with a confirmed or inspected infectious disease. (GIDXX is a placeholder code, not a final code.)
Limiting use. “We anticipate the HCPCS code GIDXX would be reported by physicians with special infectious disease training”
Can use G2211 when you use modifier 25 for an E/M and wellness visit on the same day, immunizations, and other preventive medicine services.
That’s the only exception.
CMS Extends Telehealth Flexibilities to Protect Physician Privacy.
Following staunch advocacy by the Texas Medical Association, the Centers for Medicare & Medicaid Services (CMS) will not require physicians to list their home address as a practice location on Medicare enrollment forms for another year when providing telehealth services, safeguarding their privacy and safety.
During the COVID-19 pandemic, CMS allowed physicians to offer telehealth services from their homes without reporting their home address on their Medicare enrollment. However, that flexibility was set to expire Dec. 31.
2023 Medicare Physician Fee Schedule Final Rule

On November 01, 2022, the Centers for Medicare & Medicaid Services (CMS) issued a final rule that includes updates and policy changes for Medicare payments under the Physician Fee Schedule (PFS), and other Medicare Part B issues, effective on or after January 1, 2023.
Recent Comments