Tag: Coding
UHC July Overview
Policy and protocol updates
Medical policy updates
Medical policy updates for July 2025 for the following plans: Medicare, Medicaid, Exchanges and commercial.
Reimbursement policy updates
See the latest updates for reimbursement policies.
Specialty Medical Injectable Drug program updates
See the latest updates to requirements for Specialty Medical Injectable Drugs for UnitedHealthcare members.
Pharmacy and clinical updates
Access upcoming new or revised clinical programs and implementation dates for UnitedHealthcare plans
Cigna Comm. New Reimbursement Policy for E/M
Cigna Healthcare® will implement a new reimbursement policy, Evaluation and Management Coding Accuracy (R49), to review professional claims billed with Current Procedural Terminology (CPT®) evaluation and management (E/M) codes 99204-99205, 99214-99215, and 99244-99245 for billing and coding accuracy in alignment with American Medical Association (AMA) E/M services guidelines.
Effective for dates of service on or after October 1, 2025, services may be adjusted by one level to reflect the appropriate reimbursement when the AMA guidelines are not met.
What this means to you
Cigna Healthcare will conduct periodic claim reviews to verify compliance. Based on that review, providers may be eligible to be removed from the program. Supporting documentation will be requested should we determine the established guidelines were not followed.
Reconsideration requests
Providers who believe their medical record documentation supports reimbursement for the originally submitted level for the E/M service should follow the reconsideration and appeals processes.
To request a reconsideration, please submit the customer’s full record of the encounter to the secure Cigna Healthcarefax number 833.392.2092. Should the original determination be overturned, claims will be adjusted, and an updated explanation of payment will be issued.
Administrative appeal rights are available if the original determination is upheld.
Cigna Comm. Removes 96 Codes from Prior Auth. List.
To help reduce the paperwork and time providers (and patients) spend seeking approvals for more routine services, Cigna Healthcare will remove 96 codes from the list of services that require prior authorization for dates of service on and after May 31, 2025. These codes include commonly requested cardiology, otolaryngology (ENT), and other routine services.
UHC Claims their new API makes work easier.
UnitedHealthCare’s Application Program Interface (API) is a free digital solution that automates everyday work.
Benefits of using API
- Reduces phone calls and paper
- Automates transactions on your timetable
- Distributes data faster to where you need it
- Get real‑time information
- Supports standard formats and compatible with new technology
- Maximizes efficiency and productivity through workflow integration
Why add API to your practice?
- Flexibility: Allows you to choose the data and API that fit your needs.
- Automation: Incorporates seamlessly into your workflow.
- Security: Ensures data is accessed and transferred securely
Humana
TIPS, TRICKS AND HELPS
PREAUTHORIZATON LISTS (PAL):
Lists of services and medications effective July 1, 2025, that may required preauthorization for members with Medicaid, Medicare Advantage, and dual Medicare-Medicaid coverage are now available.
Easily determine if a prior authorization is required with Humana’s search tool. Search by Current Procedural Terminology (CPT®) codes, procedures or generic drug name(s). Remember to verify benefit coverage in Availity Essentials
Availity Essentials Introduces Check Claim Status Feature:
Availity has enhanced its Eligibility and Benefits (E/B) page by adding a Check Claim Status feature.
What you can expect:
- Improved efficiency and accuracy: The check Claim Status tool pre-populates your patient’s information, ensuring accuracy.
- Time savings: You can access claim status with one click- saving time and effort
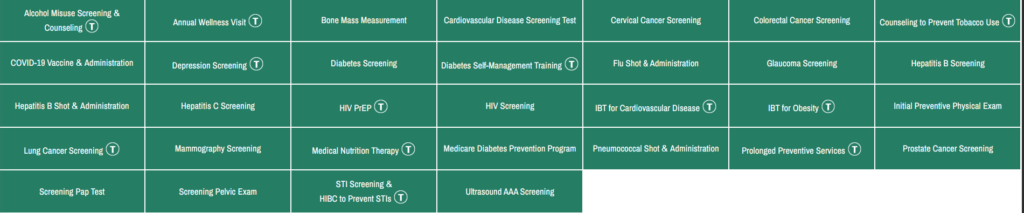
Medicare Preventive Services – Revised
The above link will lead you to MLN Educational Tool, where you can click a service and see the changes.
Aetna OfficeLink Updates May 2025
May 2025
This month’s reminders:
We regularly review and adjust our clinical, payment and coding policies. Review our policies and claim edits on our provider portal on Availity®.* Just go to Payer Space > Resources > Expanded Claim Edits. Or you may visit Aetna.com to see them.
Coding/billing update: To align with CMS, starting August 1, 2025 we’ll no longer cover 88305 (Level IV surgical pathology, gross and microscopic examination) when billed with 55700 and/or 55706 (prostate incision procedures) on the same date of service. We’ll also allow G0416 (surgical pathology, gross and microscopic examinations) once per date of service.
Note to Texas providers: Changes described in this article will be implemented for fully insured plans written in the state of Texas only if such changes are in accordance with applicable regulatory requirements. Changes for all other plans will be as outlined in this article
Billing Tips by “Physicians Practice”

- Correct Data Entry and Demographics at Check-in
Accurate data entry during patient check-in is critical. Gathering complete insurance and demographic information helps ensure proper billing and reduces potential claim denials. Make sure you always collect a photo of the patient’s insurance card, and most importantly, a photo of the back of the card. The back of the card is often more important for billing than the front.
2. Understand Your Insurance Payer Contracts.
Knowing exactly what your contract allows in terms of reimbursement rates, covered services, and billing guidelines helps prevent underpayment or denials.
3. Accurate Coding of Symptoms vs. Diagnoses.
Use the appropriate diagnosis codes for billing, avoiding the use of symptoms as primary codes. Insurance companies typically require specific diagnoses for proper reimbursement.
4. Frequent and Proactive Denials Management.
Actively follow up on denied claims and address the issues promptly. Letting accounts receivable (AR) build up can lead to financial complications and decreased revenue. Analyzing denial patterns, rectifying errors, and resubmitting claims correctly are essential steps. In particular, don’t leave denial follow ups to biweekly or monthly batched processes. The best practice is to build denials into your standard, weekly claims, and payment posting processes. In addition, the first time you receive a denial, your billing team should call the insurance payer to understand the reason behind the denial. This way, you can prevent the same error from occurring in future claims
5. Thorough Documentation.
Maintain detailed and accurate medical records for each patient. Poor documentation not only affects patient care but can also lead to audit risks and billing disputes. Proper documentation is not only required under your insurance payer contract but also required as a part of your state license as a health care practitioner.
6. Proper Secondary (2ndary) Insurance Filing.
Understand the proper procedures for filing claims with 2ndary insurance. Know the coordination of benefits (COB) and which insurance is the primary one. Often, the patient may not even be clear as to which is the primary. Have the patient contact their insurance payers and verify the primary and 2ndary insurance. Secondary payers often require physical documentation of the primary payer rejecting the claim first and this explanation of benefits (EOB) must sent along with the claim.
7. Medicare Billing Compliance.
Follow the guidelines set by Medicare’s Local Coverage Determinations (LCDs) when billing for services. Noncompliance could lead to denied claims and financial penalties.
8. Access to Insurance Portals.
Ensure you have access to the online portals of all insurance providers you work with. This will help you track claims, check eligibility, and communicate efficiently.
Aetna Fee Schedule Update Effective Today
However, Aetna tells POET the fee schedule is not ready for them to send out, yet.
CMS Enables Physicians to Bill for Secure Patient Portal Messaging.
To address this growing reliance on digital communication, CMS has updated billing policies, enabling physicians to bill for secure patient portal messaging.
This shift has led to the introduction of new CPT® codes for “e-visits,” allowing practices to capture revenue for these services:
- 99421: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 5-10 minutes
- 99422: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 11-20 minutes
- 99423: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 21 or more minutes
HCPCS code G2012 has been deleted and replaced by CPT ® code 98016, defined as:
Brief communication technology-based service (e.g., virtual check-in) by a physician or other qualified health care professional who can report evaluation and management services, provided to an established patient, not originating from a related evaluation and management service provided within the previous 7 days nor leading to an evaluation and management service or procedure within the next 24 hours or soonest available appointment, 5-10 minutes of medical discussion.
These codes allow providers to bill for longer e-visit consultations conducted through secure patient portals or other digital platforms. Key requirements include:
- An established patient-provider relationship
- Adherence to specific documentation standards that meets payer criteria
- Time-based billing for asynchronous digital evaluation initiated by patients over a seven-day period per clinical episode.
While patient portal messaging increases convenience and fosters engagement, practices must establish clear policies for appropriate use. These policies should address:
- Obtaining patient consent for e-visits
- Applying clinical judgment
- Thorough documentation in the portal message
- Adherence to payer-specific rules.
Several clinical roles could help manage the workload of patient portal messages and phone calls to relieve providers:
- Nurse practitioners (NPs) can handle many routine inquiries and provide medical advice within their scope of practice.
- Physician assistants (PAs) can address many patient concerns and questions.
- Registered nurses (RNs) can triage messages, answer general health questions, and escalate complex issues to providers.
- Clinical pharmacists can manage medication-related inquiries and provide patient education on drug interactions and side effects.
- Care coordinators can handle non-clinical questions about appointments, referrals, and care plans.
- Medical assistants can manage routine administrative tasks and simple clinical inquiries under provider supervision.
- Health coaches can address lifestyle and wellness-related questions, supporting chronic disease management.
- Patient navigators can guide patients through the healthcare system, answering questions about processes and resources.
Key aspects of successful models include:
- Selective billing: Only charging for messages requiring medical expertise and taking significant time (typically five minutes or longer)
- Tiered pricing: Adjusting costs based on insurance coverage
- Clear communication: Informing patients about which types of messages may incur charges
- Low frequency: Billing for a small percentage of total messages (often less than 1%)
Recent Comments