Month: October 2025
Medicare Beneficiaries Involved in CMS Data Breach
CMS Notifies Individuals Potentially Impacted by Data Incident
Approximately 103,000 beneficiaries may have been impacted.
POET has been told by several offices, they are seeing beneficiaries who have been assigned a new number by CMS.
CMS Instructs MACs to Lift Claims Hold

Special edition – courtesy of Novitas Solutions
Claims Hold Update
CMS instructed all Medicare Administrative Contractors (MACs) to lift the claims hold and process claims with dates of service of October 1, 2025, and later for certain services impacted by select expired Medicare legislative payment provisions passed under the Full-Year Continuing Appropriations and Extensions Act, 2025 (Pub. L. 119-4, Mar. 15, 2025). This includes claims paid under the Medicare Physician Fee Schedule, ground ambulance transport claims, and Federally Qualified Health Center (FQHC) claims. This includes telehealth claims that CMS can confirm are definitively for behavioral and mental health services. CMS has directed all MACs to continue to temporarily hold claims for other telehealth services (i.e. those that CMS cannot confirm are definitively for behavioral and mental health services) and for acute Hospital Care at Home claims.
Beginning October 1, 2025, for services that are not behavioral health services, many of the statutory limitations on payment for Medicare telehealth services that were, in response to the COVID-19 Public Health Emergency, lifted, and subsequently extended, through legislation again took effect. These include prohibition of many services provided to beneficiaries in their homes and outside of rural areas, and hospice recertifications that require a face-to-face encounter. In the absence of Congressional action, practitioners who choose to perform telehealth services that are not payable by Medicare on or after October 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage (ABN). Further information on use of the ABN, including ABN forms and form instructions: https://www.cms.gov/medicare/forms-notices/beneficiary-notices-initiative/ffs-abn. Practitioners should monitor Congressional action and may choose to hold claims associated with telehealth services that are currently not payable by Medicare in the absence of Congressional action. For further information: https://www.cms.gov/medicare/coverage/telehealth.
CMS notes that the Bipartisan Budget Act of 2018 (Pub. L. 115-123, Feb. 9, 2018), which added section 1899(l) to the Social Security Act, allows clinicians in applicable Medicare Shared Savings Program Accountable Care Organizations (ACOs) to provide and receive payment for covered telehealth services to certain Medicare beneficiaries without geographic restrictions and in the beneficiary’s home. Separate from requirements to participate in the Medicare Shared Savings Program, there is no special application or approval process for applicable ACOs or their ACO participants or ACO providers/suppliers to offer these covered telehealth services. Clinicians in applicable ACOs can furnish and receive payment for covered telehealth services under these special telehealth flexibilities. For clinicians in applicable ACOs, telehealth claims that CMS can confirm are definitively for behavioral and mental health services will be paid. At this time, claims for some telehealth services will continue to be held. For more information, including information on to which ACOs these flexibilities apply: https://www.cms.gov/files/document/shared-savings-program-telehealth-fact-sheet.pdf.
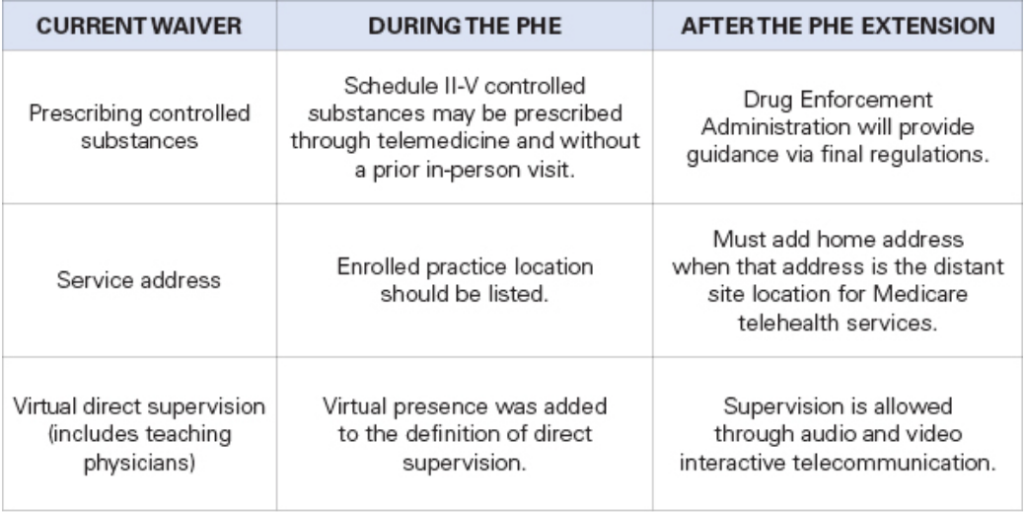
More Telehealth Waivers Set to Expire Dec. 31
As TMA monitors the government shutdown and the coinciding expiration of certain telehealth waivers as of Sept. 30, physicians should take notice of another series of telehealth waivers set to expire at the end of this year.
TMA staff note that Medicare Advantage plans don’t have to follow Medicare’s policy on the waiver expirations.
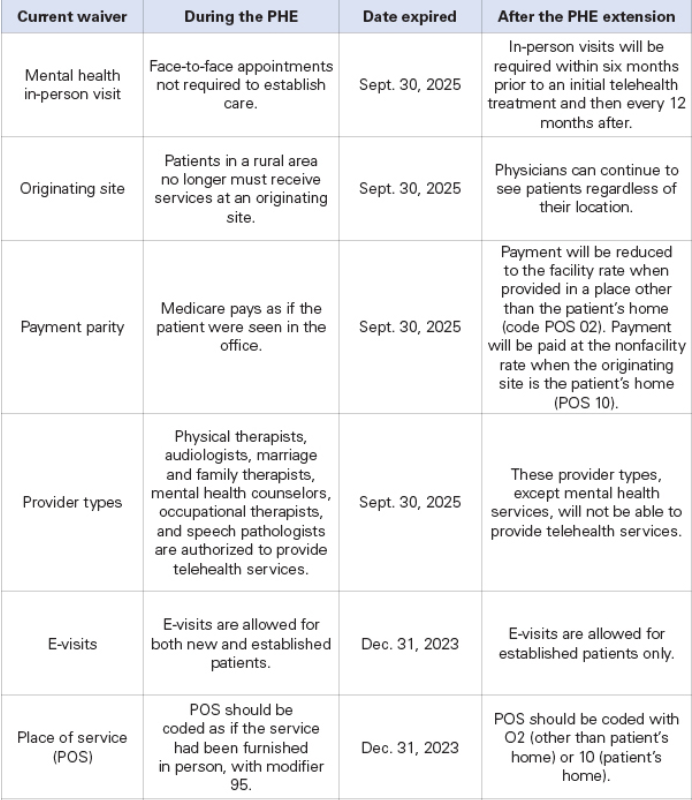
The following waivers enacted during the COVID-19 public health emergency (PHE) are currently expected to expire Dec. 31 unless Congress acts:
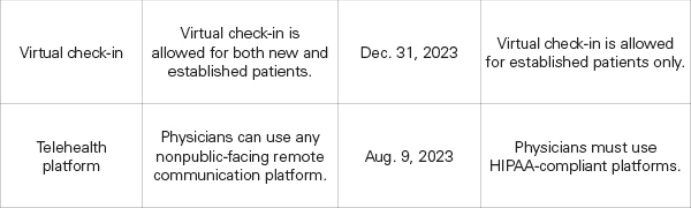
The following waivers have already expired:
TMA Coming to Tyler
Local Medicine Matters Conference Tyler, Texas
October 24-25, 2025
The Local Medicine Matters Conference is a new regional event, part of the Texas Medical Association’s initiative to hold events beyond the Texas metro areas. This inaugural conference is being hosted by the Smith County Medical Society in conjunction with TMA. The one-day event features topics of broad interest across all physician members, including practical uses of augmented intelligence in medicine, updates to billing and coding, and how physicians fared following the 2025 Texas legislative session.
Friday Night Mixer Oct. 24th
5:00 PM – 7:PM
Guest and Members Free
Saturday Conference Oct. 25th
7:30 AM – 4:00 PM
TMA Members Free
Registration
Registration for TMA members, CMS and association staff, and Alliance members is FREE – one of the many benefits of annual membership!
A $25 registration fee will be charged for on-site registrants.
Registration Fees:
Nonmember physicians: $200
Guests of members and medical staff: $150
Conference Agenda
Friday, Oct. 24 | The Grove Kitchen and Gardens
5 pm – 7 pm | Regional Membership Happy Hour
Saturday, Oct. 25 | Brookshire Conference Center
7:30 am – 1:00 pm | Registration Open
8:00 am – 8:30 am | Walk-with-A-Doc in the Tyler Rose Garden
8:15 am – 9:00 am | Breakfast
9:00 am – 9:15 am | Opening Remarks
Jayesh Shah, MD, President, Texas Medical Association
9:15 am – 10:15 am | Augmented Intelligence: Policies, Procedures, and Preparation
Explore how augmented intelligence (AI) is being practically applied in medicine to enhance efficiency and ease for healthcare professionals.
Shannon Vogel, AVP, Health Information Technology, Texas Medical Association
10:25 am – 11:25 am | P.R.O.A.C.T.I.V.E
In billing, your best practice is to be proactive. When you are reactive, payment delays, denials, and loss of revenue are more likely to occur. This presentation will review key points and best practices for being proactive to assist with efficiency and minimize unnecessary delays.
Carra Benson, Director, Physician Payment Services, Texas Medical Association
11:30 am – 12:30 pm | Lunch
12:30 pm – 1:30 pm | 2025 Legislative Wins: Texas Edition
Jayesh “Jay” Shah, MD, President, Texas Medical Association
Matt Dowling, Director of Public Affairs, Lobbyist, Texas Medical Association
1:40 pm – 2:40 pm | Lawsuits and TMB Investigations: How to Avoid Them (Ethics CME)
Lajuana Acklin, JD, Senior Associate, Bertolino Law Firm
2:50 pm -5:00 pm | Media Training
Brent Annear, Associate Vice President, Media Relations and Leadership Advancement, Texas Medical Association
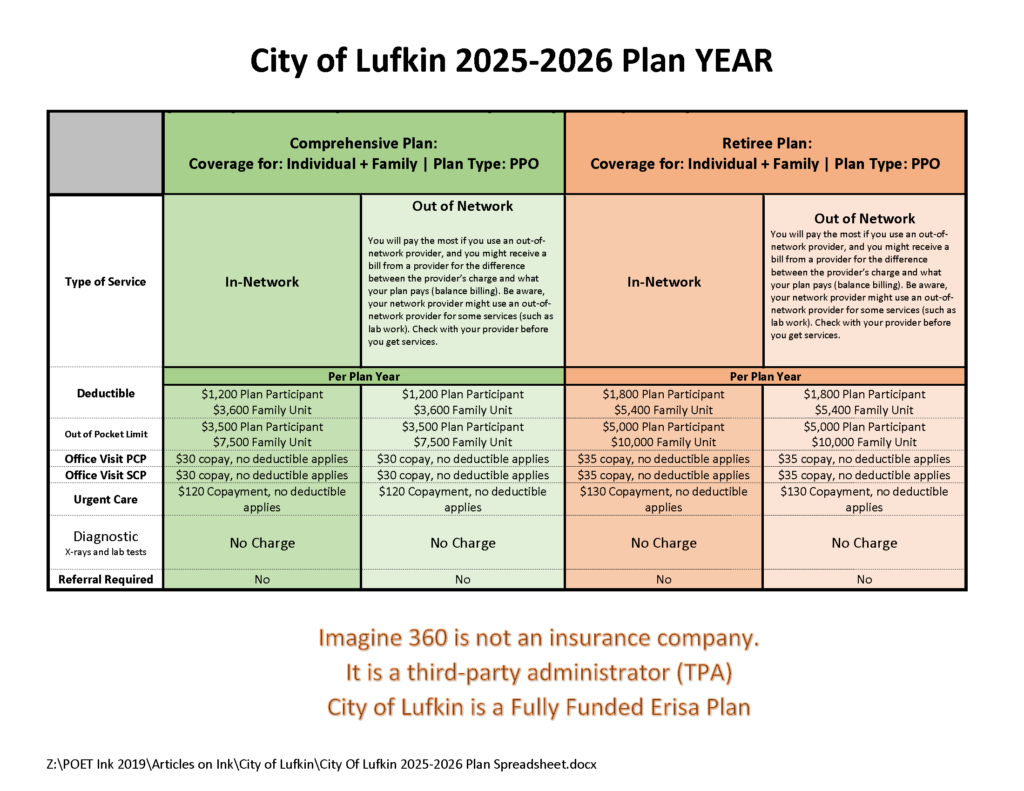
City of Lufkin 2025-2025 Benefits
Texas Law Requires Practitioners to Disclose AI Use
Texas is imposing new transparency regulations on electronic health records (EHRs) and the diagnostic use of artificial intelligence (AI) under a new state law physicians must begin complying with as of Sept. 1.
Texas Senate Bill 1188, passed during Texas’ 2025 regular legislative session, requires physicians and health care practitioners who use AI for diagnostic purposes – including for any recommendations on a diagnosis or course of treatment based on a patient’s medical records – to, effective Sept. 1:
- Disclose such use of AI to their patients; and
- Review all records created by AI in a manner consistent with medical records standards.
Additionally, entities covered by the bill – businesses, including physician practices, that assemble, collect, analyze, use, evaluate, store, or transmit protected health information – to:
- Automatically allow a minor patient’s parent, guardian, or conservator to obtain “complete and unrestricted access” to the minor’s EHR, unless access to all or part of the record is restricted under state or federal law or by court order, also effective Sept. 1; and
- Physically maintain their EHRs only within the U.S. or a territory of the U.S. and only allow their data to be accessed by those who require the information to perform duties within their scope of their job related to treatment, payment, and other health care operations by Jan. 1, 2026. Covered entities have until Jan. 1, 2026 to ensure compliance relating to EHRs prepared before Sept. 1.
However, Texas physicians are now allowed three days to communicate the results of certain sensitive or serious test results to patients, including minors and their guardians, before they are made available via EHRs thanks to the passage of Senate Bill 922.
SB 1188 also prohibits covered entities from amending on an EHR an individual’s biological sex as recorded by a health care practitioner at birth and documented in the EHR, except to correct a clerical error, or, if the individual is diagnosed with a sexual development disorder, to change the individual’s listed biological sex to the opposite biological sex, in which case, information on the disorder must be also included in the EHR.
SB 1188 states regulatory agencies – including the Texas Medical Board, the Texas Department of Licensing and Regulation, and the Texas Department of Insurance – may take disciplinary action against a covered entity that violates the order three or more times in the same manner. The disciplinary action may include “license, registration, or certification suspension or revocation for a period the agency determines appropriate,” per the law.
Violations of SB 1188 can also result in civil penalties ranging from $5,000 to $250,000 per violation, depending on the violator’s intent and whether the violator used protected health information for financial gain.
Physicians should monitor for future guidance and check with their EHR vendor about compliance, especially as related to where patient data is stored, says Shannon Vogel, the Texas Medical Association’s associate vice president of health information technology.
For more information on health information technology, visit TMA’s related webpage.
Goverment Shutdown: What you Need to Know
With the government shutdown in effect, the Texas Medical Association is in regular communication with federal colleagues at the American Medical Association on the impact to physician practices, as AMA remains in touch with senior officials at the Centers for Medicare & Medicaid Services (CMS).
The volatility in Washington, D.C. could mean the shutdown lasts days to weeks, and TMA will share additional information via Texas Medicine Today as the situation develops. Here is what physicians need to know so far:
Medicare/Medicaid: The CMS contingency plan states that during a lapse in funding, the Medicare program will continue. CMS also says it has sufficient funding for Medicaid to fund the first quarter of 2026 and is maintaining the staff necessary to make payments to eligible states for the Children’s Health Insurance Program.
Medicare Administrative Contractors (MACs) have been instructed to implement a temporary claims hold of 10 business days, which AMA says should have minimal impact on physicians due to the 14-day payment floor. “The hold prevents the need for reprocessing large volumes of claims should Congress act after the statutory expiration date,” states a CMS Medicare Learning Network Connects special edition email newsletter that, as of this writing, had not yet been publicly posted. Physicians may continue to submit claims during this period, but payment will not be released until the hold is lifted. For the latest information, AMA recommends physicians monitor their MAC’s website (Novitas in Texas) and this CMS webpage.
“In the past, Congress generally has restored lapsed policies back to the effective date of the shutdown. During the shutdown, the AMA is monitoring any potential delays in Medicare claims processing or other Medicare payment problems that could result from federal staffing reductions at CMS, including during the shutdown,” said AMA CEO and Executive Vice President John Whyte, MD, MPH.
Telehealth: Physicians who provide telehealth services to fee-for-service Medicare patients should be aware that the Medicare telehealth flexibilities lapsed on Sept. 30 for most care and congressional action is required to restore that waiver. The exceptions are patients being treated for mental health and/or behavioral health disorder (including substance use disorders), stroke, and monthly end-stage renal disease visits for home dialysis. Otherwise, telehealth services are limited to rural areas as they were before the COVID public health emergency, and patients cannot receive telehealth services in their homes. The ability to provide audio-only services to Medicare patients also lapsed, as did the Acute Hospital Care at Home program.
The CMS newsletter suggests “practitioners who choose to perform telehealth services that are not payable by Medicare on or after Oct. 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage.”
However, AMA notes physicians in certain Medicare Shared Savings Program accountable care organizations can continue to provide and be paid for telehealth services.
Other services: CMS says it is continuing federal insurance marketplace activities, such as eligibility verification. Other nondiscretionary activities including health care fraud and abuse control and Center for Medicare & Medicaid Innovation activities are also continuing.
However, AMA reports that funding extensions for community health centers, the National Health Service Corps, and teaching health centers that operate graduate medical education programs expired on Sept. 30, and the 1.0 work geographic practice cost index floor extension expired on Oct. 1. Additional programs that have lapsed include: special diabetes programs; public health emergency authorities (e.g., Public Health Emergency Fund); increased inpatient hospital payment adjustment for certain low-volume hospitals; the Medicare-Dependent Hospital program; quality measure endorsement, input, and selection; and outreach and assistance for low-income programs (e.g., area agencies on aging).
TMA wants to hear from you. If you or your practice staff experience Medicare payment delays, telehealth obstacles, or other concerns, please let us know through TMA’s Knowledge Center to help inform advocacy.
Amy Lynn Sorrel
Associate Vice President, Editorial Strategy & Programming
Division of Communications and Marketing
Government Shutdown Changes

What has changed due to the Government Shutdown?
It’s pandemic-era flexibilities that will come to an end:
- Geographic restrictions that only permitted telehealth in medically underserved areas
- Requiring the patient to go to an originating site (a health care facility) instead of being in their homes
- Allowing therapists (PTs, OTs, SLPS, audiologists) to perform services via telehealth
Behavioral health via telehealth will still be allowed after September 30th, because Congress passed a law allowing it permanently. It won’t be affected by a government shutdown, if one occurs. The Social Security Act references “mental health” as opposed to “behavioral”.
Quoting the MLN Matters Article on E/M services
MLN006764 September 2025
Telehealth Services
Section 2207 of the Full-Year Continuing Appropriations and Extensions Act, 2025, extended many of these flexibilities through September 30th, 2025. Starting October 1, 2025, the statutory limitations that were in place for Medicare telehealth services before the COVID-19 public health emergency (PHE) will retake effect for most telehealth services.
These include:
- Geographic restrictions
- Location restrictions on where you can provide services
- Limitations on the scope of practitioners who can provide telehealth services
That is, telehealth as we know it to anywhere in the country, in the patient’s home ends. How do you know if you are in an underserved area, and can continue to do telehealth? Quick and easy: could your practice do telehealth before the pandemic? Yes: in all likelihood, you can continue, but remember the patient must go to an originating site, not their homes. Are you in an underserved area? Check here.
At CodingIntel, we have a copy of the CMS telehealth fact sheet from prior to the pandemic. It isn’t up-to-date with the list below, but it will tell you the rules for most practices in the country if a shutdown occurs.
Still allowed are services that weren’t implemented as a result of the pandemic.
eCFR :: 42 CFR 410.78 — Telehealth services.
(iv) The geographic requirements specified in paragraph (b)(4) of this section do not apply to the following telehealth services:
(A) Home dialysis monthly ESRD-related clinical assessment services furnished on or after January 1st, 2019, at an originating site described in paragraphs (b)(3)(vi), (ix), or (x) of this section, in accordance with section 1881(b)(3)(B) of the Act; and
(B) Services furnished on or after January 1st, 2019, for purposes of diagnosis, evaluation, or treatment of symptoms of an acute stroke.
(C) Services furnished on or after July 1st, 2019, to an individual with a substance use disorder diagnosis, for purposes of treatment of a substance use disorder or a co-occurring mental health disorder.
(D) Services furnished on or after January 1st, 2025, for the purposes of diagnosis, evaluation, and/or treatment of a mental health disorder. Payment will not be made for a telehealth service furnished under this paragraph unless the physician or practitioner has furnished an item or service in person, without the use of telehealth, for which Medicare payment was made (or would have been made if the patient were entitled to, or enrolled for, Medicare benefits at the time the item or service is furnished) within 6 months prior to the initial telehealth service and within 6 months of any subsequent telehealth service.
Betsy
Sorry POST Missing
POET ask you to forgive us. The post in the “Latest Post” email titled “If you think 2024 was good” had to be taken down. The video of October 2024 festivities was causing a gliche.
BUT….. If you like old abandoned hospitals……
Come see 2025
Recent Comments