Tag: Current Procedural Terminology (CPT®)
HS
Updates for HealthSpring providers | |
We’re changing prior authorization requirements that may apply to some HealthSpring Medicare Advantage members. Changes are based on updates from utilization management prior authorization assessment, Current Procedural Terminology (CPT®) code changes released by the American Medical Association or Healthcare Common Procedure Coding System code changes from the Centers for Medicare & Medicaid Services. For some services and members, prior authorization may be required through HealthSpring utilization management, and related services for Medicare Advantage members will be reviewed by HealthSpring and EviCore healthcare. | |
These changes begin July 1, 2026: · Implementation of Part B Step Therapy Program · Addition of orthotic codes to be reviewed by HealthSpring · Addition of new Medicare Advantage Prescription Drug plan codes to be reviewed by HealthSpring | |
For more information, refer to the prior authorization requirements list on the clinical review page. Always check eligibility and benefits first through Availity® Essentials or your preferred vendor prior to rendering services. This step will confirm prior authorization requirements and utilization management vendors, if applicable. Checking eligibility and/or benefit information and/or obtaining prior authorization is not a guarantee of payment. Benefits will be determined once a claim is received and will be based upon, among other things, the member’s eligibility, and the terms of the member’s evidence of coverage. If you have any questions, call the number on the member’s ID card. Services performed without required prior authorization or that do not meet medical necessity criteria may be denied for payment, and the rendering provider may not seek reimbursement from the member. | |
Thank you for your partnership. | |
CPT copyright 2025 American Medical Association. All rights reserved. CPT is a registered trademark of the AMA. | |
HealthSpring products and services are provided exclusively by or through operating subsidiaries of Health Care Service Corporation, a Mutual Legal Reserve Company. PO Box 20002, Nashville, TN 37202 © Copyright 2026 Health Care Service Corporation. All Rights Reserved. |
HCPCS codes no longer requiring invoice – Avoid rejected claims
To reduce provider burden, certain contractor-priced HCPCS codes no longer require a paper invoices.
When the invoice information is entered in the narrative field on a claim for any of the HCPCS codes listed below, it is not necessary to provide the actual paper invoice for these services.
The required narrative information includes:
The dosage of the medication or the size of the biological administered.
Claims not containing information about the invoice or cost associated with the code(s) will reject as unprocessable.
Invoice amount
Enter the invoice amount in item 19 of the CMS-1500 paper claim form or the electronic equivalent using the following format (including cents):
Claim example:
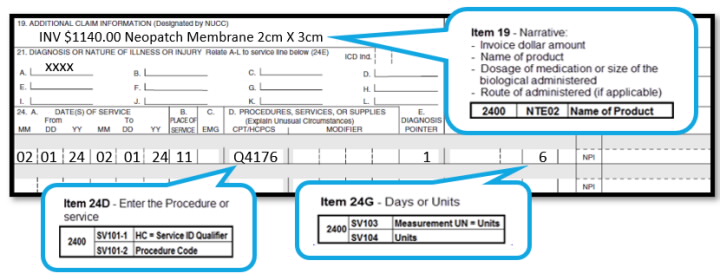
The invoice amount is the total amount a provider pays for an item/service, taking into account ALL discounts, rebates, refunds, or other adjustments to an item. You must maintain sufficient documentation in the patient’s file in the event of a review.
The evaluation of codes for this list is an ongoing process. Be sure to check back frequently and subscribe to our mailing list.
Aetna Changes in NPL
Changes in National Precertification List
As of August 1, 2025, we require precertification for the following:
- Conexxence (denosumab-bnht, J3490, J3590, C9399)
- Bomyntra (denosumab-bnht, J3490, J3590, C9399)
- denosumab-bnht (biosimaliar Prolia, J3490, J3590, C9399)
- denosumab-bnht (biosimaliar Xgeva, J3490, J3590, C9399)
- Omlyclo (omalizumab-igec, J3490, J3590, C9399) (precertification includes the site of care)
- penpulimab-kcqx (J3490, J3590, C9399) (precertification includes the site of care)
- ustekinumab-stba (J3490, J3590, C9399)
- ustekinumab (J3490, J3590, C9399)
- Starjemza (ustekinumab-hmny, J3490, J3590, C9399)
Submitting precertification requests:
Submit precertification requests at least two weeks in advance and include the actual date of service in the request. To save time, request precertification online through our provider portal on Availity.* Doing so is fast, secure and simple.
You can also use your practice’s Electronic Medical Record (EMR) system if it’s set up for electronic precertification requests. Use our “Search by CPT® code” function on our Precertification Lists page to find out if the code requires precertification.***
If you need precertification for a specialty drug for a commercial or Medicare member, submit your request through Novologix®, which is also available on Availity®.
Note to Texas providers: Changes described in this article will be implemented for fully insured plans written in the state of Texas only if such changes are in accordance with applicable regulatory requirements. Changes for all other plans will be as outlined in this article.
Cigna Comm. Removes 96 Codes from Prior Auth. List.
To help reduce the paperwork and time providers (and patients) spend seeking approvals for more routine services, Cigna Healthcare will remove 96 codes from the list of services that require prior authorization for dates of service on and after May 31, 2025. These codes include commonly requested cardiology, otolaryngology (ENT), and other routine services.
Medicare Preventive Services – Revised
The above link will lead you to MLN Educational Tool, where you can click a service and see the changes.
Aetna OfficeLink Updates May 2025
May 2025
This month’s reminders:
We regularly review and adjust our clinical, payment and coding policies. Review our policies and claim edits on our provider portal on Availity®.* Just go to Payer Space > Resources > Expanded Claim Edits. Or you may visit Aetna.com to see them.
Coding/billing update: To align with CMS, starting August 1, 2025 we’ll no longer cover 88305 (Level IV surgical pathology, gross and microscopic examination) when billed with 55700 and/or 55706 (prostate incision procedures) on the same date of service. We’ll also allow G0416 (surgical pathology, gross and microscopic examinations) once per date of service.
Note to Texas providers: Changes described in this article will be implemented for fully insured plans written in the state of Texas only if such changes are in accordance with applicable regulatory requirements. Changes for all other plans will be as outlined in this article
CMS Enables Physicians to Bill for Secure Patient Portal Messaging.
To address this growing reliance on digital communication, CMS has updated billing policies, enabling physicians to bill for secure patient portal messaging.
This shift has led to the introduction of new CPT® codes for “e-visits,” allowing practices to capture revenue for these services:
- 99421: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 5-10 minutes
- 99422: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 11-20 minutes
- 99423: Online digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 21 or more minutes
HCPCS code G2012 has been deleted and replaced by CPT ® code 98016, defined as:
Brief communication technology-based service (e.g., virtual check-in) by a physician or other qualified health care professional who can report evaluation and management services, provided to an established patient, not originating from a related evaluation and management service provided within the previous 7 days nor leading to an evaluation and management service or procedure within the next 24 hours or soonest available appointment, 5-10 minutes of medical discussion.
These codes allow providers to bill for longer e-visit consultations conducted through secure patient portals or other digital platforms. Key requirements include:
- An established patient-provider relationship
- Adherence to specific documentation standards that meets payer criteria
- Time-based billing for asynchronous digital evaluation initiated by patients over a seven-day period per clinical episode.
While patient portal messaging increases convenience and fosters engagement, practices must establish clear policies for appropriate use. These policies should address:
- Obtaining patient consent for e-visits
- Applying clinical judgment
- Thorough documentation in the portal message
- Adherence to payer-specific rules.
Several clinical roles could help manage the workload of patient portal messages and phone calls to relieve providers:
- Nurse practitioners (NPs) can handle many routine inquiries and provide medical advice within their scope of practice.
- Physician assistants (PAs) can address many patient concerns and questions.
- Registered nurses (RNs) can triage messages, answer general health questions, and escalate complex issues to providers.
- Clinical pharmacists can manage medication-related inquiries and provide patient education on drug interactions and side effects.
- Care coordinators can handle non-clinical questions about appointments, referrals, and care plans.
- Medical assistants can manage routine administrative tasks and simple clinical inquiries under provider supervision.
- Health coaches can address lifestyle and wellness-related questions, supporting chronic disease management.
- Patient navigators can guide patients through the healthcare system, answering questions about processes and resources.
Key aspects of successful models include:
- Selective billing: Only charging for messages requiring medical expertise and taking significant time (typically five minutes or longer)
- Tiered pricing: Adjusting costs based on insurance coverage
- Clear communication: Informing patients about which types of messages may incur charges
- Low frequency: Billing for a small percentage of total messages (often less than 1%)
BCBSTX no longer paying for Consults
Effective 11/18/2024
If you missed it, check out the article posted 9/4/2024
“BCBSTX to Require E/M Codes for Consultation Services”
BCBSTX to Require E/M Codes for Consultation Services
Starting Nov. 18, Blue Cross and Blue Shield of Texas (BCBSTX) will no longer pay physicians for outpatient or inpatient consultations when they report those services with Current Procedural Terminology (CPT) codes 99242 – 99245 and 99252 – 99255.
Instead, the payer says physicians will need to report consultation services with an appropriate office outpatient or inpatient evaluation and management (E/M) code representing where the visit occurred and its level of complexity.
According to the health plan, consultation claims reported with CPT codes after Nov. 18 will be denied.
Updated 12/10/2024, to add BCBS website information
Evaluation and Management Coding – Professional Provider Services
Policy Number: CPCP024
Version 1.0
Enterprise Clinical Payment and Coding Policy Committee Approval Date:
August 7, 2024
Plan Effective Date: November 18, 2024
(Blue Cross and Blue Shield of Texas Only
Consultation(s) CPT Codes 99242-99245 ,99252-99255 Effective 11/18/2024, the plan will no longer reimburse for office/outpatient consultation codes (CPT codes 99242–99245) and inpatient consultation codes (CPT codes 99252–99255). Consultation services should be reported with an appropriate office/outpatient or inpatient E/M code representing the location where the visit occurred and the level of complexity of the visit performed, such as code ranges 99221-99223, 99304-99306, and 99202-99215.
Good News, Bad News in Medicare 2025
A first look at the 2025 Physician Fee Schedule
The 2025 Physician Fee Schedule proposed rule is a study in contrasts. If you’re the kind of person who can see both sides of an issue, this rule is for you.
Good News
Bad News
Practitioners doing telehealth from their home can continue to use the practice address instead of their home address on claims for 2025
Without an act of Congress, for real time audio/visual visits on 1/1/2025 patients can no longer receive these services in their homes in all geographic areas. Patients must be in an underserved area and go to a facility setting for telehealth. (Unless Congress changes this in their end of year Consolidated Appropriations Act.)
16 new telehealth codes that can be selected based on Medical Decision Making (MDM) or time.
Medicare has given them a status indicator of invalid.
New HCPCS code for GIDXX for visit complexity inherent to in patient and observation services associated with a confirmed or inspected infectious disease. (GIDXX is a placeholder code, not a final code.)
Limiting use. “We anticipate the HCPCS code GIDXX would be reported by physicians with special infectious disease training”
Can use G2211 when you use modifier 25 for an E/M and wellness visit on the same day, immunizations, and other preventive medicine services.
That’s the only exception.
Recent Comments