Tag: Novitas Solutions
Who Would’ve Thought?
Novitas Training on YouTube!
Novitas has made learning more convenient by offering helpful tutorials on YouTube. These short videos provide quick guidance on common Medicare topics, making it easier to find answers without having to attend a full webinar.
Goverment Shutdown: What you Need to Know
With the government shutdown in effect, the Texas Medical Association is in regular communication with federal colleagues at the American Medical Association on the impact to physician practices, as AMA remains in touch with senior officials at the Centers for Medicare & Medicaid Services (CMS).
The volatility in Washington, D.C. could mean the shutdown lasts days to weeks, and TMA will share additional information via Texas Medicine Today as the situation develops. Here is what physicians need to know so far:
Medicare/Medicaid: The CMS contingency plan states that during a lapse in funding, the Medicare program will continue. CMS also says it has sufficient funding for Medicaid to fund the first quarter of 2026 and is maintaining the staff necessary to make payments to eligible states for the Children’s Health Insurance Program.
Medicare Administrative Contractors (MACs) have been instructed to implement a temporary claims hold of 10 business days, which AMA says should have minimal impact on physicians due to the 14-day payment floor. “The hold prevents the need for reprocessing large volumes of claims should Congress act after the statutory expiration date,” states a CMS Medicare Learning Network Connects special edition email newsletter that, as of this writing, had not yet been publicly posted. Physicians may continue to submit claims during this period, but payment will not be released until the hold is lifted. For the latest information, AMA recommends physicians monitor their MAC’s website (Novitas in Texas) and this CMS webpage.
“In the past, Congress generally has restored lapsed policies back to the effective date of the shutdown. During the shutdown, the AMA is monitoring any potential delays in Medicare claims processing or other Medicare payment problems that could result from federal staffing reductions at CMS, including during the shutdown,” said AMA CEO and Executive Vice President John Whyte, MD, MPH.
Telehealth: Physicians who provide telehealth services to fee-for-service Medicare patients should be aware that the Medicare telehealth flexibilities lapsed on Sept. 30 for most care and congressional action is required to restore that waiver. The exceptions are patients being treated for mental health and/or behavioral health disorder (including substance use disorders), stroke, and monthly end-stage renal disease visits for home dialysis. Otherwise, telehealth services are limited to rural areas as they were before the COVID public health emergency, and patients cannot receive telehealth services in their homes. The ability to provide audio-only services to Medicare patients also lapsed, as did the Acute Hospital Care at Home program.
The CMS newsletter suggests “practitioners who choose to perform telehealth services that are not payable by Medicare on or after Oct. 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage.”
However, AMA notes physicians in certain Medicare Shared Savings Program accountable care organizations can continue to provide and be paid for telehealth services.
Other services: CMS says it is continuing federal insurance marketplace activities, such as eligibility verification. Other nondiscretionary activities including health care fraud and abuse control and Center for Medicare & Medicaid Innovation activities are also continuing.
However, AMA reports that funding extensions for community health centers, the National Health Service Corps, and teaching health centers that operate graduate medical education programs expired on Sept. 30, and the 1.0 work geographic practice cost index floor extension expired on Oct. 1. Additional programs that have lapsed include: special diabetes programs; public health emergency authorities (e.g., Public Health Emergency Fund); increased inpatient hospital payment adjustment for certain low-volume hospitals; the Medicare-Dependent Hospital program; quality measure endorsement, input, and selection; and outreach and assistance for low-income programs (e.g., area agencies on aging).
TMA wants to hear from you. If you or your practice staff experience Medicare payment delays, telehealth obstacles, or other concerns, please let us know through TMA’s Knowledge Center to help inform advocacy.
Amy Lynn Sorrel
Associate Vice President, Editorial Strategy & Programming
Division of Communications and Marketing
HCPCS codes no longer requiring invoice – Avoid rejected claims
To reduce provider burden, certain contractor-priced HCPCS codes no longer require a paper invoices.
When the invoice information is entered in the narrative field on a claim for any of the HCPCS codes listed below, it is not necessary to provide the actual paper invoice for these services.
The required narrative information includes:
The dosage of the medication or the size of the biological administered.
Claims not containing information about the invoice or cost associated with the code(s) will reject as unprocessable.
Invoice amount
Enter the invoice amount in item 19 of the CMS-1500 paper claim form or the electronic equivalent using the following format (including cents):
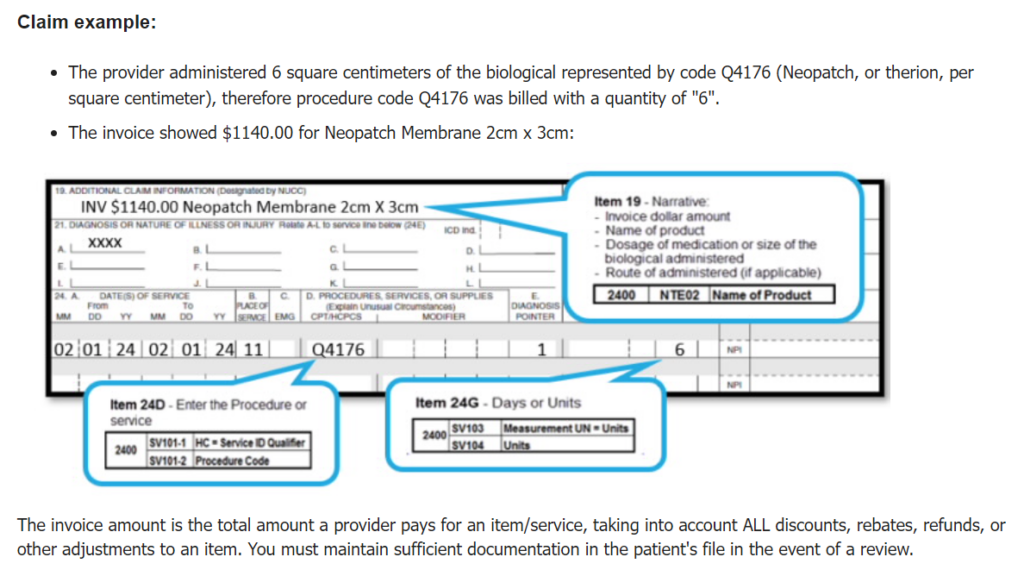
Claim example:
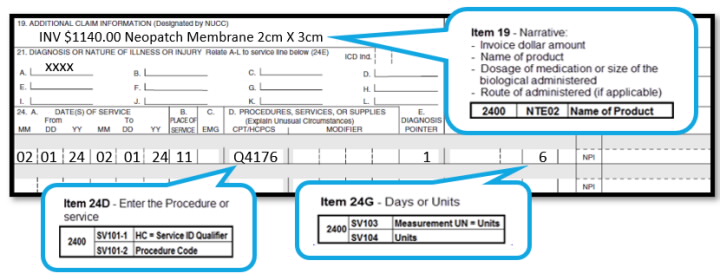
The invoice amount is the total amount a provider pays for an item/service, taking into account ALL discounts, rebates, refunds, or other adjustments to an item. You must maintain sufficient documentation in the patient’s file in the event of a review.
The evaluation of codes for this list is an ongoing process. Be sure to check back frequently and subscribe to our mailing list.
Modifier 25 Fact Sheet from Novitas
Modifier 25 Fact Sheet
Modifier 25 is defined as a significant, separately identifiable evaluation and management (E/M) service by the same physician or other qualified health care professional on the same day of a procedure or other service.
Physicians of the same specialty in the same group practice are considered the same physician; therefore, they must bill and be paid as though they were a single physician.
Appropriate Use
Use modifier 25 with the appropriate level of E/M service.
- Modifier 25 indicates on the day of a procedure, the patient’s condition required a significant, separately identifiable E/M service, above and beyond the usual pre- and post-operative care associated with the procedure or service performed.
- E/M service may occur on the same day as a procedure. Medicare allows payment when the documentation supports modifier 25.
- A minor surgical procedure performed has a global period of 0-day or 10-day listed on the Medicare physician fee schedule (JH) (JL) and meets the definition of modifier 25.
Global Surgery
Global surgery is defined as all necessary services normally furnished by a surgeon before, during, and after a procedure. Medicare payment for a surgical procedure includes pre-operative, intra-operative, and post-operative services routinely performed by the surgeon or by members of the same group with the same specialty.
Do not use modifier 25 when billing for services performed during a post-operative period if related to the previous surgery. Related follow-up examinations by the same provider during the global period of a previous procedure are included in that procedure’s global surgical package.
- For an unrelated E/M service during the global period of a previous procedure, you may be able to report an appropriate E/M code with modifier 24 (unrelated evaluation and management service by the same physician during a postoperative period) appended.
- The E/M is for a new problem not related to the patient’s previous complaint or procedure.
- Append modifier 57 (decision for surgery), rather than modifier 25, if the E/M service prompts the decision to render a major procedure within 24 hours of the E/M service. Major procedure is defined as one with a 90-day global period.
National Correct Coding Initiative (NCCI) Procedure-to-procedure (PTP) edits
The NCCI promotes national correct coding methodologies and controls improper coding leading to inappropriate payment. The PTP code pair edits are automated prepayment edits preventing improper payment when reporting certain codes together for Part B-covered services on the same day by the same physician.
When both correct coding and global surgery edits apply to the same claim by the same physician, we’ll first apply the correct coding edits. Then, we’ll apply the global surgery edits to the correctly coded services
References:
E/M visit complexity add-on HCPS code G2211,
Effective for dates of service on and after January 1, 2025:
HCPCS code G2211 is payable when an associated office and outpatient (O/O) E/M base code (CPT codes 99202-99205 or 99211-99215) is reported with modifier 25 for the same patient by the same provider and a Part B preventive service, immunization administration, or annual wellness visit service identified in attachment 1 in Change Request (CR) 13705 is also present for the same date of service.
For claims not containing one of the identified services above or dates or service prior to January 1, 2025:
- Claims will deny when HCPCS code G2211 and an associated office and outpatient (O/O) E/M visit (CPT codes 99202-99205 or 99211-99215) is reported with modifier 25 for the same patient by the same provider on the same date of service:
- Separately identifiable visits occurring on the same day as minor procedures (such as 0 or 10-day global procedures) have resources sufficiently distinct from costs associated with furnishing stand-alone O/O E/M visits to justify different payment.
References:
- Change Request 13705 – Allow Payment for Healthcare Common Procedure Coding System (HCPCS) Code G2211 when Certain Part B Preventive Services are Provided on the Same Day
- MLN Matters article MM13473 – How to Use the Office & Outpatient Evaluation and Management Visit Complexity Add-on-Code G2211
- MLN Matters article MM13272 – Edits to Prevent Payment of G2211 with Office/Outpatient Evaluation and Management Visit and Modifier 25c
Inappropriate use
Avoid denials of claims with an appropriate use of modifier 25
- Do not report HCPCS code G2211 when modifier 25 is reported on an associated E/M visit (CPT codes 99202-99205 and 99211-99215) for claims not containing a Part B preventive service, immunization administration, or annual wellness visit service or dates of service prior to January 1, 2025.
- Do not use modifier 25 on HCPCS code G2211.
- Do not use modifier 25 on CPT code 99211
- Do not use modifier 25 by a physician other than the physician performing the procedure or physician of the same specialty in the same group practice.
- Do not use modifier 25 when documentation does not support a significant, separately identifiable E/M service.
References:
- CMS IOM Pub. 100-04 Medicare Claims Processing Manual, Chapter 12, section 40.2-40.5
- CMS IOM Pub. 100-04 Medicare Claims Processing Manual, Chapter 23, section 30.2
- E/M Service-specific coding instructions
- Frequently Asked Questions: Evaluation and management services
- Global Surgery Fact Sheet
- Global surgery & related services
- Global surgery calculator (JH) (JL)
- Local contractor pricing references
- MLN Matters article MM13452 – Medicare Physician Fee Schedule Final Rule Summary: CY 2024
- Modifier 25 tip sheet
Have Questions About Capturing Telehealth Visits?
Teleheath appears to become increasingly complex on a daily basis.
The following is a list of guidelines provided by MGMA:
Click on the title to follow the link.
Smart Edits are Going Away
Smart Edits were introduced in July of 2023 to analyze claim data and will be removed effective June 28th. No action is needed. The removal of these edits will not impact your electronic billing routine. The typical workday using electronic billing will remain the same.
Your Mac is Novitas Solutions
Today, HHS is announcing immediate steps that the Centers for Medicare & Medicaid Services (CMS) is taking to assist providers to continue to serve patients. CMS will continue to communicate with the health care community and assist, as appropriate. Providers should continue to work with all their payers for the latest updates on how to receive timely payments.
Medicare providers needing to change clearinghouses that they use for claims processing during these outages should contact their Medicare Administrative Contractor (MAC) to request a new electronic data interchange (EDI) enrollment for the switch. The MAC will provide instructions based on the specific request to expedite the new EDI enrollment. CMS has instructed the MACs to expedite this process and move all provider and facility requests into production and ready to bill claims quickly. CMS is strongly encouraging other payers, including state Medicaid and Children’s Health Insurance Program (CHIP) agencies and Medicaid and CHIP managed care plans, to waive or expedite solutions for this requirement
CMS has contacted all of the MACs to make sure they are prepared to accept paper claims from providers who need to file them. While we recognize that electronic billing is preferable for everyone, the MACs must accept paper submissions if a provider needs to file claims in that method.
Novitas Phone # (855) 252-8782. Have your PTAN and the last 5 of your TIN.
Change HealthCare!

Looking for answers? So is POET. We are looking for work-arounds. Hopefully we will have some up before closing today.
Prevent Improper Code Bundling
Physicians can take advantage of a new Medicare tool to sort through service codes that can be bundled together for claims payment – and AVOID improper billing.
The CMS recently released the National Correct Coding Initiative (NCCI) procedure-to-procedure (PTP) lookup tool to promote accurate code-bundling and prevent improper payment of Medicare Part B and Medicaid claims when incorrect code combinations are reported.
Available via Texas’ Medicare contractor Novitas Solutions, the tool is further designed to help physicians identify when certain pairs of codes are subject to automated edits.
AND FOR EVEN MORE TOOLS
CLICK ON ANY OF THE BUTTONS BELOW
Recent Comments