Tag: Billing/Coding
ERISA or maybe TPA?
Let’s play pretend:
Some one gives you this card and wants to make an appointment.
They seem to want an answer right now.
You know your physician takes Blue Choice, but have never seen this card before. How would you know?
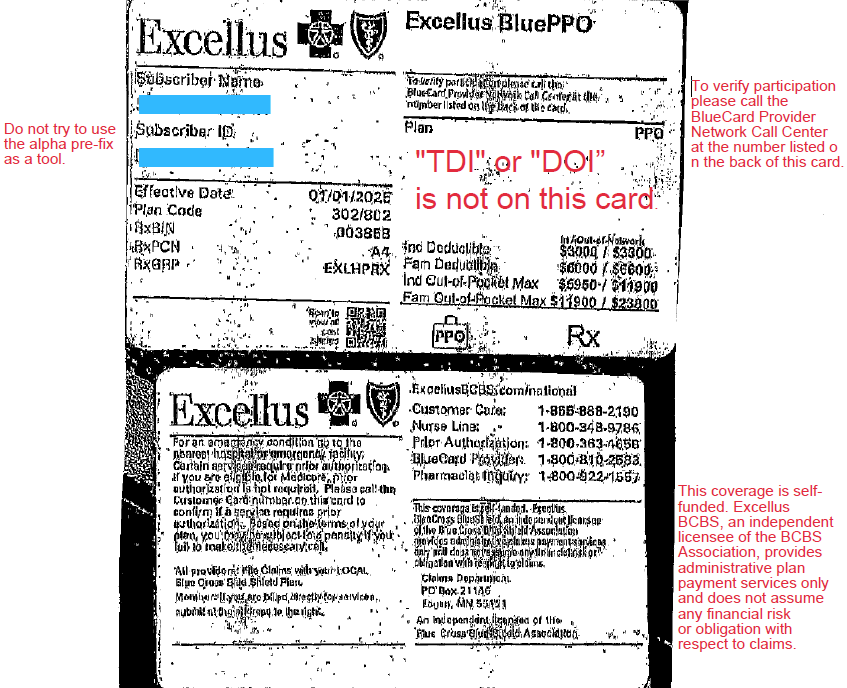
Look at the front of the card. Blue Cross is written all over it. BCBS must be the insurer? STOP!
Do you see any insurance regulation language? Is “TDI” or “DOI” on this card?
NO. This is your 1st clue. The employer may be the insurer.
Scan the front of the card intently. Are there any other clues. Look for what you know, not what you don’t know.
If not flip it over. What do you see? READ ALL THE TINY WRITING.
On this card: phone numbers, addresses, where to file, prior auth info. But what else?
“This coverage is self-funded Excellus BlueCross BlueShield, and independent licensee of the BlueCross BlueShield Association provides administrative claims payment services only and does not assume any financial risk or obligation with respect to claims.”
What does that mean:
- The employer is the insurer (self-funded plan)
- Excellus BCBS is acting as a Third-Party Administrator (TPA)
Is this a Lease Network?
Very likely — yes.
On the front of the card it says:
“To verify participation, please call the BlueCard Provider Network.”
That suggests:
- The plan is using the BlueCard network
- Excellus is providing network access + claims processing. The employer is leasing the BCBS network
That’s what we commonly call a lease network arrangement.
But — this is important — don’t assume, Verify
Why you may still get a “Yes” when you call
When you call provider services:
- The rep may simply see “In Network”
- They may not understand lease networks
- They may not understand the difference between:
- Payor
- TPA
- Repricer
- Network administrator
So we need to ask better questions.
Instead of just asking “Is Dr. Smith in network?”
Tell the representative you would like to check network participation.
Ask:
- Is this plan self-funded? (if it is self-funded it is not a lease network)
- Is Excellus the payor, or the administrator?
- Is this a leased network?
- Who bears the financial risk?
- Is Excellus repricing the claims?
- What network applies to this patient?
And always get:
✔ Representative name
✔ Date/time
✔ Call reference number
If the claim denies, that reference number becomes your leverage.
Why this matters
In lease network plans:
- The employer controls the benefits.
- The employer may carve out services.
- The employer may override network rules.
- The plan can be patient-specific.
Basically they can make up their own rules.
In practical terms — They have more flexibility than a fully insured DOI-regulated plan.
Protect Yourself when speaking to the patient.
Never speak in absolutes.
Use language like:
- “It looks like this is a self-funded plan…”
- “Based on the card wording…”
- “According to the representative I spoke with…”
- “At the time of verification…”
Never say:
- “Yes, you are definitely covered.”
- “This will pay.”
- “You are in network.”
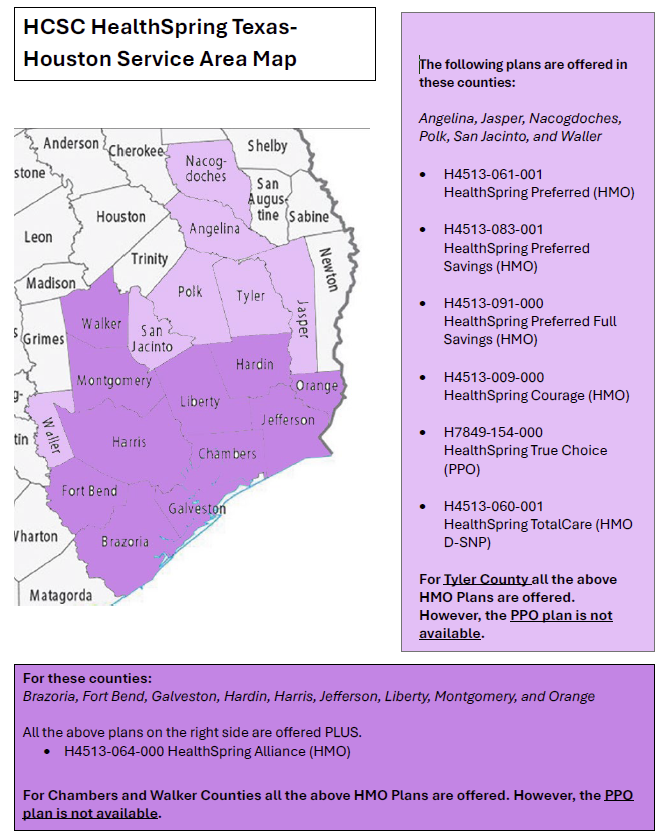
HealthSpring Plans by County
POET staff has done everything short of a full skeletal reconstruction to make the HealthSpring county page in the provider manual legible. They’ve stretched it. They’ve shrunk it. They’ve even converted it to Word and back to a PNG. It just didn’t have the backbone it needed.
If we were tibia honest, nothing worked.
So I, Sir Seymore Bones — resident WordPress writer and part-time osteo-optimizer — took pen in hand (metacarpals and all) to give everyone a little relief. When the formatting started rattling, I decided it was time to get to the bare bones of the issue.
I hope the map below helps you Sey-more, and make sense of the plans offered in our counties. We femur-ly believe this version is better. If it doesn’t… well, I promise I didn’t bone it up on purpose.
Stay humerus,
Sir Seymore Bones
CMS-1500 vs Electronic Claims (837P)
What is a HCFA anyway?
POET understands, not everyone is a biller, and we might be throwing out alphabet soup to some office personal.
What is a CMS-1500 (HCFA) Form?
The CMS-1500, often still called a HCFA, is the standard paper form used to bill insurance companies for professional services provided by physicians and other healthcare providers.
It tells the insurance company:
Who the patient is
Who the provider is
What services were performed
When the services occurred
Why they were medically necessary
How much is being charged
What is Used When Claims Are Filed Electronically?
When an office files claims electronically, the equivalent of the CMS-1500 form is an: ANSI 837P Claim
837 = electronic claim format
P = Professional services
The 837P contains the same information as a CMS-1500, just in a computer-readable format instead of paper.
Why Staff May Not “See” an 837P
The billing software creates it automatically
It is sent through a clearinghouse
Insurance companies process it behind the scenes
Most staff interact with screens and reports, not the actual electronic file.
If You Need to See a “Paper Copy” of an 837P
An 837P does not have a true paper form. However, billing systems can produce a claim print image or CMS-1500-style report that shows the same data contained in the electronic claim.
This is often called:
Claim print image
CMS-1500 claim view
Electronic claim summary
These reports are used for: (Why POET would request it)
Reviewing what was sent
Troubleshooting rejections or denials
Sharing claim details with non-billing staff
Important: This is a readable representation of the 837P data — not the actual electronic file.
To see the raw 837P file itself, billing staff would need to export or view it through the billing system or clearinghouse.
Disclaimer: The information provided in this blog is for general educational purposes only. While Ink strives to explain insurance concepts accurately and clearly, payer rules, contracts, and policies can vary widely by plan, state, and provider agreement—and they change frequently.
This content should not be interpreted as definitive guidance or a substitute for reviewing payer manuals, contracts, or official communications. Physician offices are encouraged to conduct their own research and verify requirements directly with the applicable insurance carriers before making operational or billing decisions.
NEW BCBSTX fee schedule coming
ATTENTION PROVIDERS
BCBSTX has notified POET that a NEW Fee Schedule for Blue Choice and Blue Essentials will be effective May 1, 2026.
Once POET receives the new fee schedule and completes its review, OPT-IN / OPT-OUT packets will be sent to physician offices for participation decisions.
Please watch for additional communication once the review process is complete
HealthSpring has a New Payor ID
PAYOR ID: 52192
Claims Address for paper claims: P.O. Box 23456 Chattanooga, TN. 37421
More on HealthSpring and CPL
Update: POET has been advised that the issue involving HealthSpring, CPL, and Polk County is related to a claims system error. HealthSpring has confirmed that they are currently in contract with CPL, and the issue is actively being worked on.
POET we keep you updated, as we receive information.
CPL Labs and HealthSpring
Just in from HealthSpring!
In Polk County, CPL Labs are not in network.
HealthSpring patients in Polk County should go to Quest or LabCorp.
BCBS Pharmacy Qtrly Updates for January 2026
Pharmacy Program Quarterly Update Changes Effective Jan. 1, 2026 – Part 1
The Definition of G0136 is Changing
Another Great Article from CodingIntel
November 2025
|
Highlights for Aetna OfficeLink Updates
Claim and Code Review Program (CCRP) update
Starting December 1, you might see new claim edits
This update applies to both our commercial and Medicare members.
Beginning December 1, 2025, you may see new claim edits. These are part of our CCRP. These edits support our continuing effort to process claims accurately for our commercial, Medicare and Student Health members. You can view these edits on our provider portal on Availity.
For coding changes, go to Aetna Payer Spaces > Resources. In the search bar, search for “expanded claim edits.”
Except for Student Health, you’ll also have access to our code edit lookup tools. To find out if our new claim edits will apply to your claim, log in to Availity®. You’ll need to know your Aetna® provider ID number (PIN) to access our code edit lookup tools.
We may request medical records for certain claims, such as high-dollar claims, implant claims, anesthesia claims, and bundled services claims, to help confirm coding accuracy.
Changes to our National Precertification List (NPL)
These changes apply to our commercial and Medicare members, unless otherwise noted.
Effective January 1, 2026, we’ll require precertification for the following:
• Electrophysiological (EP) study (93654)
• Yondelis® (trabectedin, J9352)
• Docivyx™ (docetaxel, J9172) — Medicare members only
Check out the Original Publication, titles like:
- How to secure an authorization
- Urgent requests
- Changes to commercial drug lists begin on January 1
- And More
Recent Comments