Administration of influenza vaccine inside a patient’s home; reported only once per individual home per date of service when such vaccine administration(s) are performed at the patient’s home
■ Important Updates for Physician Offices-New Plans Coming in 2026
New benefit plans under the HealthSpring name will roll out January 2026. For now, you can find articles about these changes on: MedicareProviders.Cigna.com …and in the Provider Newsroom.
■ Claims Contact Information
Jim Denman will no longer handle claims. For more information, please call POET
■ Goodbye HSConnect – Hello Availity Essentials
Cigna MA has partnered with Availity Essentials for enhanced online tools. HSConnect and Cigna for HCP are no longer needed.
■ Verify eligibility & benefits ■ Verify primary care provider ■ View customer ID cards ■ View maximum-out-of-pocket amounts ■ Submit professional & institutional claims ■ Check claim status
■ View remittance advice ■ Access Cigna MA links (including prior authorizations & resources) via the Payer Space page
The Texas Health and Human Services Commission (HHSC) will transition Medicaid-only services for dually eligible clients (eligible for both Medicare and Medicaid) from Fee-for-Service (FFS) to a Managed Care service delivery system.
Superior HealthPlan will be responsible for adjudicating these claims.
Provider Responsibilities
Submit claims for Medicaid-only services for dual eligible clients directly to the Managed Care Organization (MCO).
If a Claim is Sent to TMHP in Error:
TMHP will forward the claim to the correct MCO.
The TMHP response will only confirm forwarding – no ER&S report will be issued.
Claims with dates of service on or after Sept. 1, 2025 will not be adjudicated by TMHP.
Provider Action Steps
✅ Submit Medicaid-only service claims directly to the MCO. ✅ Contact the MCO for claim status and adjudication questions. ✅ Review the Rider 32 Procedure Code List (PDF) for impacted services. ✅ Reach out to your Provider Representative via the Find My Provider Representative webpage.
Addressing physician concerns about online Medicaid enrollment challenges, the Texas Medicaid and Healthcare Partnership (TMHP) has announced its new Provider Enrollment Assistant Tool (PEAT) is available for enrollment-related help.
Users can navigate to the help page in TMHP’s provider enrollment section to access the tool, which TMHP describes as “question-based software.” Typing in a question prompts PEAT to provide:
Answers to revalidation questions, including due dates;
Online appointment scheduling for personalized support with enrollment issues, including step-by-step guidance from a TMHP representative;
Information about Provider Enrollment and Management System (PEMS) maintenance requests; and
Instructions for new enrollments, re-enrollments, and updates to existing enrollments.
Before initiating a PEAT request, TMHP advises having at the ready your National Provider Identifier (NPI), ZIP code, taxonomy number (if applicable), and any contact information related to the NPI.
In addition to a PEAT info sheet accessible online, TMHP is offering walk-through sessions for those needing additional enrollment support, which can be scheduled via PEAT, and offers an online PEMS guide updated in March.
To reduce provider burden, certain contractor-priced HCPCS codes no longer require a paper invoices.
When the invoice information is entered in the narrative field on a claim for any of the HCPCS codes listed below, it is not necessary to provide the actual paper invoice for these services.
The required narrative information includes:
Invoice dollar amount and quantity for the drug or biological.
Name of the drug or biological administered.
The dosage of the medication or the size of the biological administered.
The route of administration if applicable.
Claims not containing information about the invoice or cost associated with the code(s) will reject as unprocessable.
Invoice amount
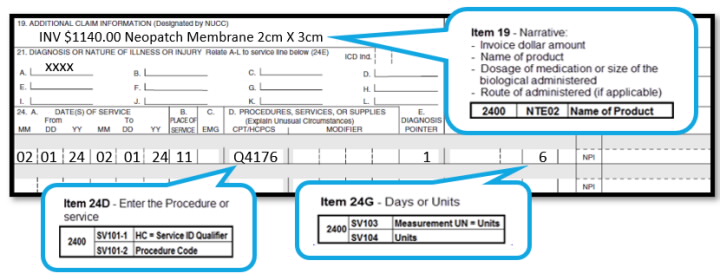
Enter the invoice amount in item 19 of the CMS-1500 paper claim form or the electronic equivalent using the following format (including cents):
Inv. $00.00 for list product name, description/size, quantity per invoice.
Claim example:
The provider administered 6 square centimeters of the biological represented by code Q4176 (Neopatch, or therion, per square centimeter), therefore procedure code Q4176 was billed with a quantity of “6”.
The invoice showed $1140.00 for Neopatch Membrane 2cm x 3cm:
The invoice amount is the total amount a provider pays for an item/service, taking into account ALL discounts, rebates, refunds, or other adjustments to an item. You must maintain sufficient documentation in the patient’s file in the event of a review.
The evaluation of codes for this list is an ongoing process. Be sure to check back frequently and subscribe to our mailing list.
Check out these essential insights on controlling malpractice insurance premiums, including specialty impact, location factors, policy types and available discounts for physicians.
Malpractice insurance is one of the largest fixed costs a physician faces — yet most doctors have no idea how their premiums are calculated, why they fluctuate, or what they can do to control them. In this article, we’re breaking down the key factors that go into determining your malpractice premium and sharing insider tips every physician should know when it comes to evaluating costs.
1. Specialty is king
The single biggest factor influencing your malpractice premium is your specialty. High-risk specialties like neurosurgery, OB/GYN, and orthopedic surgery typically carry much higher premiums than lower-risk fields such as dermatology or psychiatry.
Within each specialty, most carriers also use subspecialty classifications to further define risk — such as “no surgery,” “minor surgery,” or “major surgery”. These distinctions matter and can significantly impact pricing.
Tip: If you practice in multiple specialties or have a hybrid role, be sure your policy reflects your actual scope of services. You may be able to structure your coverage in a way that reduces your premium while still protecting your full scope of work.
2. Location, location, location
Your practice location(s) play a major role in how your malpractice premium is calculated. Not only do rates vary by state, but even different counties within the same state can carry dramatically different pricing based on local claim frequency and severity. If you’re practicing in more than one location — whether through telemedicine, locums, or a multi-site practice — the premium will be influenced by the rating in each location and the percentage of time you practice there.
Underwriters typically apply a blended rate or assign a primary territory based on where the majority of your work occurs, but if one of your locations is in a high-risk region, it can drive the cost up significantly.
Tip: If you’re considering adding a new practice location or accepting work in another state, talk to your broker before committing. A good broker can help you get preliminary premium estimates and show you how the coverage may be rated based on your time spent in each place — helping you avoid surprises and make an informed decision.
3. Policy type: Occurrence vs. claims-made
The type of policy you choose – Occurrence vs. Claims-Made – has a significant impact on your premium. Occurrence policies tend to be more expensive upfront but include automatic tail coverage. Claims-made policies are usually cheaper in the early years but require a separate tail policy once you cancel the coverage.
Tip: Claims-made premiums increase gradually over time, typically maturing over 5 years. If you’re reviewing a first-year quote, ask for projections for future years so you’re not surprised by the standard step increases — which are often mistaken for price hikes. Also, plan ahead for tail coverage, which usually costs 150–200% of the mature premium and is paid as a lump sum when the policy ends.
4. Policy Limits Matter — But Not as Much as You Think
While your coverage limits (e.g., $1 million/$3 million) do affect premium, the price difference between standard limit options is often marginal. What matters most is that your limits are appropriate — not too low and not unnecessarily high.
Too-low limits can leave you exposed if a claim exceeds your policy’s maximum payout. In these cases, any excess judgment could become a personal financial liability. On the other hand, excessively high limits can sometimes attract unwanted attention from plaintiff attorneys, who may be more aggressive when they believe there’s a “deep pocket” to pursue.
Tip: Aim for the right-size coverage based on your specialty, location, and risk profile. Your limits should satisfy state requirements and credentialing standards, while also aligning with your actual exposure. A trusted broker can help you find that balance and avoid over- or under-insuring your practice.
5. Claims history and risk profile
A physician’s personal claims history, board actions, or disciplinary issues can impact their ability to obtain favorable coverage — and often result in surcharges or placement with a non-standard carrier.
However, this is not always permanent. Many carriers are willing to reconsider a provider’s risk profile after a few stable years. If no new claims or issues arise, physicians can often transition back into the standard market and begin receiving preferred pricing again within 3 to 5 years.
Tip: If you’ve experienced a claim or board action, don’t assume it’s the end of the road. A knowledgeable broker can help you find short-term solutions and guide you toward long-term recovery — positioning you for a return to standard coverage as your risk profile improves.
6. Discounts and credits
Many physicians are eligible for premium discounts based on factors like part-time status, new-to-practice classification, risk management participation, and more. These credits are typically nondiscretionary — meaning that if you qualify, the carrier is required to apply them.
However, it’s up to you and your broker to ensure the insurer has all the correct information. Carriers won’t apply discounts they don’t know you qualify for. That’s why it’s important to clearly explain your work setup and keep your broker informed of any changes throughout the year. In some cases, additional savings may be available for professional affiliations, clean claims history, or procedural specifics — but only if your broker knows to ask.
Tip: Keep your broker in the loop about how your practice is structured and any updates as they happen. A good broker will proactively look for all eligible discounts — but they can only advocate for what they know.
Final thought: The importance of shopping around
Not all carriers calculate premiums the same way. Two companies could quote very different rates for the exact same provider — especially if they classify your risk differently or apply different credits. This is why it’s critical to shop the market — not just at renewal, but anytime your practice evolves.
Malpractice insurance is too important to set and forget. Whether you’re changing jobs, expanding your scope, or just want peace of mind, regularly reviewing your coverage ensures you’re getting the right protection at the right price — without paying for more than you actually need.
Jennifer Wiggins is the CEO and Founder of Aegis Malpractice Solutions, an independent malpractice insurance brokerage that helps physicians across the country find the best coverage for their unique practice needs. She also hosts the podcast “Malpractice Insights,” offering free education and real-world guidance for health care providers navigating malpractice insurance.
Omlyclo (omalizumab-igec, J3490, J3590, C9399) (precertification includes the site of care)
penpulimab-kcqx (J3490, J3590, C9399) (precertification includes the site of care)
ustekinumab-stba (J3490, J3590, C9399)
ustekinumab (J3490, J3590, C9399)
Starjemza (ustekinumab-hmny, J3490, J3590, C9399)
Submitting precertification requests:
Submit precertification requests at least two weeks in advance and include the actual date of service in the request. To save time, request precertification online through our provider portal on Availity.* Doing so is fast, secure and simple.
You can also use your practice’s Electronic Medical Record (EMR) system if it’s set up for electronic precertification requests. Use our “Search by CPT® code” function on our Precertification Lists page to find out if the code requires precertification.***
If you need precertification for a specialty drug for a commercial or Medicare member, submit your request through Novologix®, which is also available on Availity®.
Note to Texas providers: Changes described in this article will be implemented for fully insured plans written in the state of Texas only if such changes are in accordance with applicable regulatory requirements. Changes for all other plans will be as outlined in this article.
New Benefit Plans will roll out under the HealthSpring (HS) name during the 2025 Annual Enrollment Period (AEP)
Beginning in 2026, you will see members enrolled in HealthSpring benefit plans. But until then physician staff and HS will continue to communicate through the Cigna Healthcare Channels, including the Provider Newsroom.
In September of this year (2025) HS will add a home page for providers. After that HS will continue to add resources to prepare the physician office and HS members for January 2026. Check out HealthSpring.com

Recent Comments