The class action lawsuit, In re: Blue Cross Blue Shield Antitrust Litigation, addresses Provider Plaintiffs’ claim that the Settling Defendants violated antitrust laws by illegally dividing the United States into “Service Areas” and agreeing not to compete in those areas. Provider Plaintiffs also claim that the Settling Defendants fixed prices for services provided. The class action is pending in the United States District Court for the Northern District of Alabama, Southern Division. U.S. District Judge R. David Proctor is overseeing it. Both sides want to avoid the risk and cost of further litigation and have agreed to the Settlement. The Provider Plaintiffs and their attorneys think the Settlement is best for the Settlement Class.
This Settlement Class includes all Providers in the U.S. (except Excluded Providers FAQ 5, who are not part of the Settlement Class) who currently provide or provided healthcare services, equipment or supplies to any patient who was insured by, or was a Member of or a beneficiary of, any plan administered by any Settling Individual Blue Plan from July 24, 2008 to October 4, 2024 (“Settlement Class Period”). Class Members who submit a valid approved claim (“Authorized Claimants”) will receive a payment from the Net Settlement Fund if the Settlement is approved
To visit the official platform Portal for Settlement Class Members to submit claims for a share of the Net Settlement Fund and to get up-to-date information about the Settlement Program. Follow the link below.
“We might have new claim edits for our commercial members.
Beginning March 1, 2025, you may see new claim edits. These are part of our CCRP. These edits support our continuing effort to process claims accurately for our commercial members. You can view these edits on our provider portal on Availity.*
For coding changes, go to Aetna Payer Space > Resources > Expanded Claim Edits
You’ll also have access to our code edit lookup tools. To find out if our new claim edits will apply to your claim, log in to our provider portal on Availity. You’ll need to know your Aetna® provider ID number (PIN) to access our code edit lookup tools.
We may request medical records for certain claims, such as high-dollar claims, implant claims, anesthesia claims, and bundled services claims, to help confirm coding accuracy.”
EHRs are increasingly leading to malpractice lawsuits. While EHR-related lawsuits still make up only a small number of lawsuits, user error is the cause of 64 percent of EHR-related malpractice claims, according to the Doctors Company. Practices need to focus on eliminating several common problems, mostly tied to user actions, which have led to the majority of EHR-related suits
Many doctors are tempted to copy a note from a prior encounter and make changes as appropriate. This leads to a few potential problems.
“Sometimes physicians forget to update the note with the appropriate changes when copying and pasting” David Troxel, MD, MeD & Sec. Doctor’s Company Brd. of Gov.
Drop-down menus can often be the source of a user error that leads to a malpractice suit. Not only can users click the wrong thing in the menu, such as the wrong patient symptom, but these menus lead to structured information that physicians can easily overlook when reviewing a note
Jeffrey Kagan, MD, a Newington, Ct.-based internist, has experience reviewing malpractice cases for attorneys. One trend he has seen related to EHR-induced malpractice suits comes from template use.
“Templates are supposed to help us do something more comprehensive, but often our templates have a lot of old information that carries forward,” he says. In order to avoid falling into this trap, He advises physicians to proofread and modify templates.
The e-prescribing module in an EHR is a potential landmine for malpractice. Alerts indicating when there is a problem with medication dosage or drug-drug interaction will pop up as practitioners are inputting data into the EHR. As a result, doctors get annoyed and develop alert fatigue, and they just turn the alerts off. While this is understandable, turning off the alerts could mean a potential significant problem could go undetected.
Another prompt that goes ignored, often to the determinant of the patient and the doctor, are clinical decision support (CDS) alerts. These are clinically relevant educational materials that come up as the practitioner is documenting in the EHR. Practitioners should ignore these at their own peril, Troxel says. If anything, physicians should document the reason why they overrode the CDS alert.
The idea of physicians missing a vital piece of information in the EHR can be either a user or a technical error. These types of problems are most likely to crop up when a physician is using a new system.
Physicians Practice: November 11, 2024, By Keith A Reynolds
How would you characterize your prior authorization experience in the last year?
We’re doing more prior authorizations
74%
We’re doing fewer prior authorizations
4%
Prior authorizations are about the same
22%
Do you think there should be a CPT code requiring payers to reimburse for prior authorization work?
Yes
97%
No
3%
What is your biggest challenge with your biggest payer?
Current systems don’t interact well with our billing systems requiring office staff to correct claims leading to delayed payment
Reimbursement stinks. I Quit !!!!!!
Staff the insurance companies contracted are mostly out of the country and do not know the issues we have and do not like to refer the questions or specific issues to any expert in the field.
Small practice is ignored. They would not negotiate fees. For more than 15 years no increase in fees, only steady decrease. It is a shame, no respect any longer for providers.
Prior authorizations waste so much time for what should be a simple process
Lack of urgency or even motivation to provide basic service
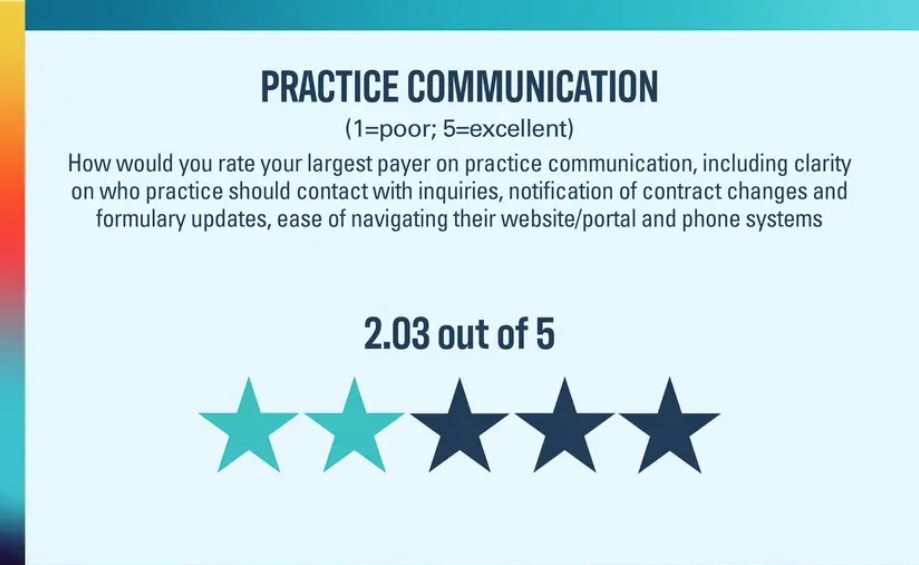
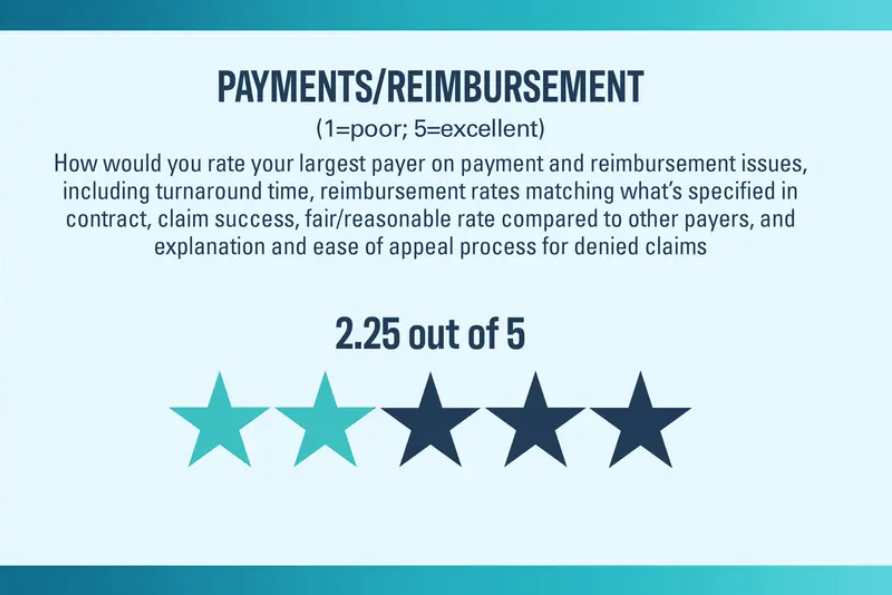
The verdict is in for how practices feel about their payers, and it isn’t good.
How can payers improve their relationship with practices?
Streamline systems to allow for clean claims the first time
Have a dedicated Provider Relations contact so we know who to talk to, and who to call to get responses to critical questions, not have to send emails to faceless representatives that have a low rate of resolution.
Communicate. Show WHY they deny, and what EXACTLY can be done to help the patients who pay them. Do not simply deny with NO guidance.
Pay us enough to survive. Instead, they raise hospital payments. Paying us more so we could hire more doctors and physicians assistants and keep people OUT of those hospitals.
Stop putting technology problems and carrier losses on the provider and their patients.
Instead of looking at me as an expense, look at me as a tool to care for their beneficiaries.
Stop requiring PAs for generic meds and obviously necessary medications.
This playbook will provide strategies to organizational leaders to enhance processes, implement time-saving workflows, increase the efficiency of their practice, and improve physician well-being
POINTS OF INTEREST:
The Burnout Problem Is Organizational, Not Personal
Stop the Unnecessary Work
Getting Rid of Stupid Stuff
Share the Necessary Work
Advanced Rooming and Discharge
Tasks Medical Assistants or Other Team Member Can Complete
Make the Case to Leadership
And Much, Much More: Graphs, podcast, practical tools, checklist, and toolkits
Every business, especially a medical practice, needs to run like a well-oiled machine
Just as oil prevents an engine from drying out and freezing up, your medical practice must have a well-developed denial management program in place. This is the first proactive step.
The shift towards digital solutions has had a profound impact and benefit. However, it has also introduced new challenges, particularly concerning security, which is why your frontline employees need to be properly trained to ensure your business and customers are protected.
As frontline sectors continue to embrace technology, the dependency on digital tools and platforms grows. Employees now rely on various devices and software to perform their duties, from processing transactions and managing customer interactions to accessing sensitive information. Point-of-sale systems, digital customer service platforms, electronic health records, and mobile apps are now standard tools in these environments.
The Importance of Security Training for Frontline Workers
Frontline workers extend beyond emergency responders. It’s an encompassing term to describe individuals who are the first point-of-contact between a company and its customers. They can handle sensitive information, greet patrons as they enter facilities, or provide direct support when needed
Why is front line training so vital?
Direct Customer Interaction
Protecting Sensitive Information
Identifying Threats
Compliance with Regulations
Building Customer Trust
For Additional Helps and Tips Visit: Vector Security’s Security Blog.
Instead, the payer says physicians will need to report consultation services with an appropriate office outpatient or inpatient evaluation and management (E/M) code representing where the visit occurred and its level of complexity.
According to the health plan, consultation claims reported with CPT codes after Nov. 18 will be denied.
Updated 12/10/2024, to add BCBS website information
Evaluation and Management Coding – Professional Provider Services
Policy Number: CPCP024
Version 1.0
Enterprise Clinical Payment and Coding Policy Committee Approval Date:
August 7, 2024
Plan Effective Date: November 18, 2024
(Blue Cross and Blue Shield of Texas Only
Consultation(s) CPT Codes 99242-99245 ,99252-99255 Effective 11/18/2024, the plan will no longer reimburse for office/outpatient consultation codes (CPT codes 99242–99245) and inpatient consultation codes (CPT codes 99252–99255). Consultation services should be reported with an appropriate office/outpatient or inpatient E/M code representing the location where the visit occurred and the level of complexity of the visit performed, such as code ranges 99221-99223, 99304-99306, and 99202-99215.








Recent Comments