Starting December 1, you might see new claim edits
This update applies to both our commercial and Medicare members.
Beginning December 1, 2025, you may see new claim edits. These are part of our CCRP. These edits support our continuing effort to process claims accurately for our commercial, Medicare and Student Health members. You can view these edits on our provider portal on Availity.
For coding changes, go to Aetna Payer Spaces > Resources. In the search bar, search for “expanded claim edits.”
Except for Student Health, you’ll also have access to our code edit lookup tools. To find out if our new claim edits will apply to your claim, log in to Availity®. You’ll need to know your Aetna® provider ID number (PIN) to access our code edit lookup tools.
We may request medical records for certain claims, such as high-dollar claims, implant claims, anesthesia claims, and bundled services claims, to help confirm coding accuracy.
Changes to our National Precertification List (NPL)
These changes apply to our commercial and Medicare members, unless otherwise noted.
Effective January 1, 2026, we’ll require precertification for the following:
• Electrophysiological (EP) study (93654)
• Yondelis® (trabectedin, J9352)
• Docivyx™ (docetaxel, J9172) — Medicare members only
Check out the Original Publication, titles like:
How to secure an authorization
Urgent requests
Changes to commercial drug lists begin on January 1
TMA’s billing, coding, and payment page offers resources for physician practices, from one end of the continuum to the other. Educate yourself with our articles and tools, or get help with more complex questions.
Physician Payment Resource Center
TMA’s Physician Payment Resource Center (formerly known as the Hassle Factor Log and the Reimbursement, Review and Resolution Service) goes to bat for members by helping to resolve issues related to insurance payments.
TMA can help resolve issues with your payer network status, prompt-pay, and other reimbursement claims. Learn More
Billing and Coding Hotline
Speak directly with TMA’s certified coders and staff experts about regulatory compliance, billing and coding, payment, and licensure concerns.
When a patient leaves your office with a referral slip, it should represent the start of seamless specialty care. Too often, though, the process falls apart. Patients forget to schedule, specialists never send notes back, or documentation gaps raise liability concerns. The result? Fragmented care, frustrated patients, and potential revenue leakage for your practice. By rethinking how referrals are handled, physicians and administrators can strengthen continuity of care, reduce risks, and make the process smoother for everyone involved. Here are five strategies to tighten up your referral process.
Standardize your referral protocols.
Without a consistent system, referrals can become a patchwork of individual physician habits. Establishing clear protocols, such as using a referral checklist or template, helps reduce variation and improves reliability. Standardization also supports quality initiatives and payer requirements. One practice leader told Physicians Practice that creating uniform workflows was key to making sure payers actually paid for the care provided, underscoring the financial upside of consistency
Referrals don’t have to be based on gut instinct or habit alone. Practices can use analytics to weigh outcomes data, proximity, and even HEDIS scores when deciding which specialist to send patients to. This kind of data-driven approach has been shown to reduce unnecessary costs and improve patient satisfaction.
Artificial intelligence is starting to take on a supportive role in referral management. For example, some health systems are testing AI models that prescreen referral requests and flag the ones most likely to need urgent specialist care. That means physicians can focus attention on complex cases while routine referrals move more efficiently.
Improve communication and tracking with colleagues
Even the best referral can fail if the patient never makes the appointment—or if the referring doctor never sees the specialist’s notes. Research shows nearly a third of patients over 65 never follow through with their referrals. Better communication between practices, whether through shared EHR systems, referral dashboards, or simple follow-up calls, can close that loop.
Liability issues around referrals often stem from documentation—or the lack of it. Recording why you referred, what diagnostic steps came first, and whether you received and reviewed the specialist’s notes is crucial. Some practices use a “rule of three,” referring only after three visits without resolution, to provide consistency and documentation clarity.
Administration of influenza vaccine inside a patient’s home; reported only once per individual home per date of service when such vaccine administration(s) are performed at the patient’s home
■ Important Updates for Physician Offices-New Plans Coming in 2026
New benefit plans under the HealthSpring name will roll out January 2026. For now, you can find articles about these changes on: MedicareProviders.Cigna.com …and in the Provider Newsroom.
■ Claims Contact Information
Jim Denman will no longer handle claims. For more information, please call POET
■ Goodbye HSConnect – Hello Availity Essentials
Cigna MA has partnered with Availity Essentials for enhanced online tools. HSConnect and Cigna for HCP are no longer needed.
■ Verify eligibility & benefits ■ Verify primary care provider ■ View customer ID cards ■ View maximum-out-of-pocket amounts ■ Submit professional & institutional claims ■ Check claim status
■ View remittance advice ■ Access Cigna MA links (including prior authorizations & resources) via the Payer Space page
The Texas Health and Human Services Commission (HHSC) will transition Medicaid-only services for dually eligible clients (eligible for both Medicare and Medicaid) from Fee-for-Service (FFS) to a Managed Care service delivery system.
Superior HealthPlan will be responsible for adjudicating these claims.
Provider Responsibilities
Submit claims for Medicaid-only services for dual eligible clients directly to the Managed Care Organization (MCO).
If a Claim is Sent to TMHP in Error:
TMHP will forward the claim to the correct MCO.
The TMHP response will only confirm forwarding – no ER&S report will be issued.
Claims with dates of service on or after Sept. 1, 2025 will not be adjudicated by TMHP.
Provider Action Steps
✅ Submit Medicaid-only service claims directly to the MCO. ✅ Contact the MCO for claim status and adjudication questions. ✅ Review the Rider 32 Procedure Code List (PDF) for impacted services. ✅ Reach out to your Provider Representative via the Find My Provider Representative webpage.
Addressing physician concerns about online Medicaid enrollment challenges, the Texas Medicaid and Healthcare Partnership (TMHP) has announced its new Provider Enrollment Assistant Tool (PEAT) is available for enrollment-related help.
Users can navigate to the help page in TMHP’s provider enrollment section to access the tool, which TMHP describes as “question-based software.” Typing in a question prompts PEAT to provide:
Answers to revalidation questions, including due dates;
Online appointment scheduling for personalized support with enrollment issues, including step-by-step guidance from a TMHP representative;
Information about Provider Enrollment and Management System (PEMS) maintenance requests; and
Instructions for new enrollments, re-enrollments, and updates to existing enrollments.
Before initiating a PEAT request, TMHP advises having at the ready your National Provider Identifier (NPI), ZIP code, taxonomy number (if applicable), and any contact information related to the NPI.
In addition to a PEAT info sheet accessible online, TMHP is offering walk-through sessions for those needing additional enrollment support, which can be scheduled via PEAT, and offers an online PEMS guide updated in March.
To reduce provider burden, certain contractor-priced HCPCS codes no longer require a paper invoices.
When the invoice information is entered in the narrative field on a claim for any of the HCPCS codes listed below, it is not necessary to provide the actual paper invoice for these services.
The required narrative information includes:
Invoice dollar amount and quantity for the drug or biological.
Name of the drug or biological administered.
The dosage of the medication or the size of the biological administered.
The route of administration if applicable.
Claims not containing information about the invoice or cost associated with the code(s) will reject as unprocessable.
Invoice amount
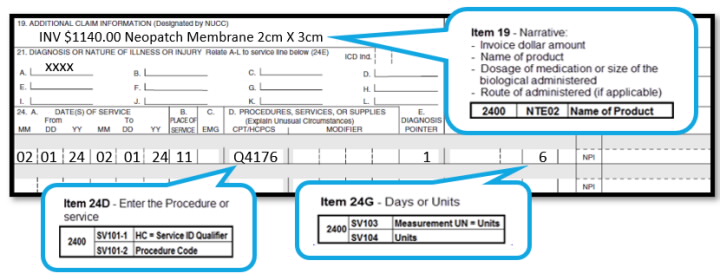
Enter the invoice amount in item 19 of the CMS-1500 paper claim form or the electronic equivalent using the following format (including cents):
Inv. $00.00 for list product name, description/size, quantity per invoice.
Claim example:
The provider administered 6 square centimeters of the biological represented by code Q4176 (Neopatch, or therion, per square centimeter), therefore procedure code Q4176 was billed with a quantity of “6”.
The invoice showed $1140.00 for Neopatch Membrane 2cm x 3cm:
The invoice amount is the total amount a provider pays for an item/service, taking into account ALL discounts, rebates, refunds, or other adjustments to an item. You must maintain sufficient documentation in the patient’s file in the event of a review.
The evaluation of codes for this list is an ongoing process. Be sure to check back frequently and subscribe to our mailing list.

Recent Comments