~Claire Ernst J.D. Government Affairs Director MGMA
On March 15, 2022, President Biden signed the $1.5 trillion omnibus spending package into law, which extended certain telehealth flexibilities related to the PHE. The following waivers will be in effect for an additional 151 days following the conclusion of the PHE:
Originating site and geographic location: Patients can continue to be treated via telehealth anywhere, including their homes
Qualifying providers: Physical therapists, occupational therapists, speech language pathologists, and audiologists can furnish distant site telehealth services
Audio-only services: CMS must continue covering and reimbursing these services
Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs): FQHCs and RHCs can be distant sites and be reimbursed
As a reminder, the PHE is in effect until April 16, 2022. It is likely that it will be renewed at least one more time for 90 days.
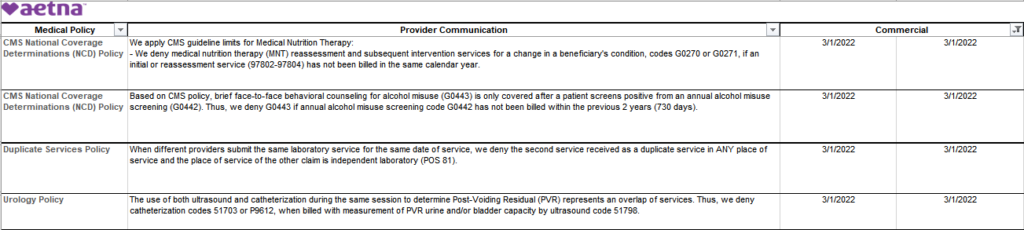
Beginning June 1, 2022, you may see new claim edits.
According to March 1, 2022 Aetna OfficeLink Updates: These are part of our Third-Party Claim and Code Review Program. These edits support our continuing effort to process claims accurately for our commercial, Medicare and Student Health members. You can view these edits on our Availity provider portal.*
You can view any of these edits on Aetna’s Availity® provider portal.
For coding changes, go to:
Aetna Payer Space
Resources
Expanded Claim Edits
Except for Student Health, you’ll also have access to Aetna’s code edit lookup tools. To find out if our new claim edits will apply to your claim, log in to our Availity provider portal. You’ll need to know your Aetna® provider ID number (PIN) to access our code edit lookup tools
Don’t cross your fingers or bring your rabbit foot.
Just download, print and keep a current copy of POET’s Provider Roster and Directory at your desk to make the Referral and Authorization process a bit easier.
Published 2/25/2022, Written by Kelsey Hagg, Associate Director Government Affairs MGMA
“In late 2021, the Texas Medical Association filed a lawsuit against the U.S. Department of Health and Human Services (HHS) alleging that the interim final rule establishing the qualifying payment amount (QPA) as the assumed out-of-network rate went against congressional intent and stating that all criteria (including the QPA) considered by the independent dispute resolution (IDR) entity should be weighted equally.
This morning a federal judge in Texas issued a motion for summary judgement ruling in favor of the Texas Medical Association.
The court determined that HHS violated the Administrative Procedures Act (APA) when issuing rulemaking establishing the QPA as the assumed out-of-network rate in the federal IDR process. This ruling means that if the higher courts don’t overturn or pause implementation pending appeals, we expect the IDR process to begin without the portions of the rule that were vacated.
Specifically, we expect the IDR process to begin without the QPA as the established out-of-network amount. Under this ruling, IDR entities do not have to select the payment amount that is closest to the QPA, nor do IDR entities have to describe the credible information that determined the QPA was materially different from the chosen out-of-network rate.
Additionally, we wanted to share information we received from CMS. In a call with the agency, a CMS spokesperson stated that they intend to open the federal IDR portal on Monday, February 28, 2022. However, this information is subject to change and we will keep you posted on any additional information we receive from the agency. Questions for CMS about the federal IDR process can be directed to: [email protected].
Please let us know if you have any additional questions.
Stand up a bonus program aligned with practice goals.
According to Evan Saulino, MD, PhD, a family physician and regional medical director at Aledade, the key is aligning value-based care work with your practice’s payment structure so staff members realize how their daily activities support quality care goals. “This also keeps the team focused on what they can do and not frustrated by what they can’t do,” Dr. Saulino said.
Some organizations award annual bonuses using a simple percentage, while others take a more nuanced approach. Dr. Saulino recommends incentivizing team members who are involved in value-based care work and who have completed a minimum tenure at the practice (e.g. a year of service). At the Walker Clinic, the bonus program unites clinical and nonclinical team members in tackling a given quality measure (e.g., mammograms), which is assigned a biannual bonus payment value. According to Walker, it’s this cross-functional alignment that’s been key to the clinic achieving shared savings.
“We all have to be on the same page and moving in a fluid motion, or we’re just not going to get there,” Walker said.



Recent Comments