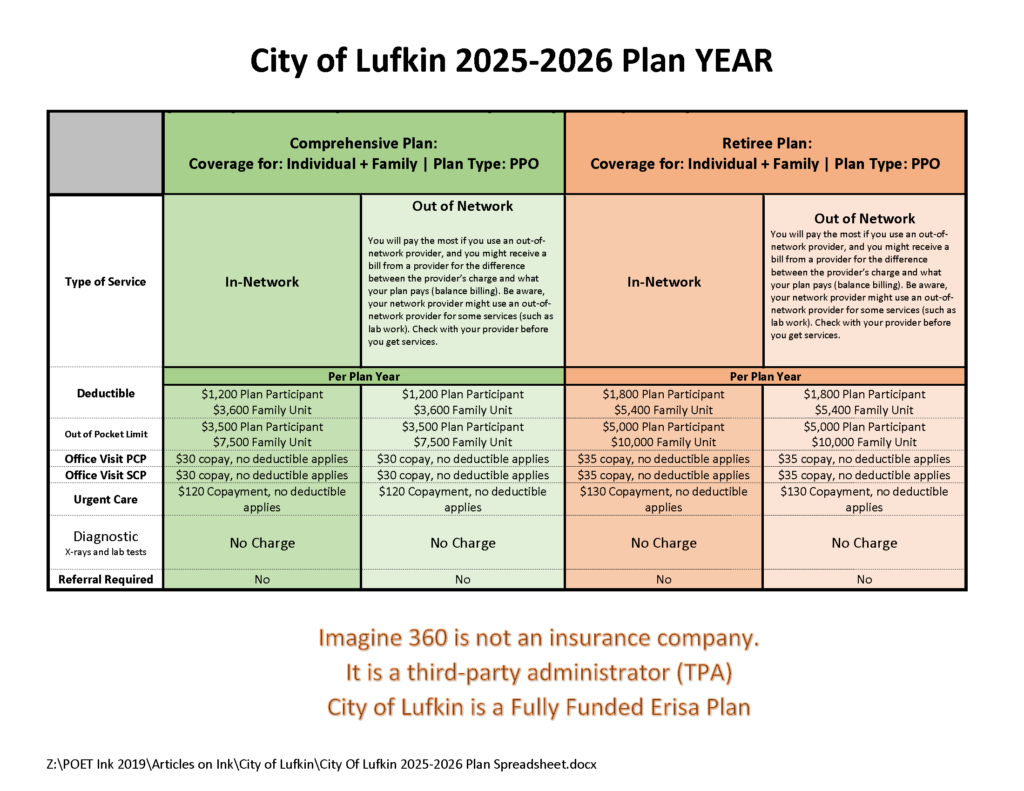
City of Lufkin 2025-2025 Benefits
Texas Law Requires Practitioners to Disclose AI Use
Texas is imposing new transparency regulations on electronic health records (EHRs) and the diagnostic use of artificial intelligence (AI) under a new state law physicians must begin complying with as of Sept. 1.
Texas Senate Bill 1188, passed during Texas’ 2025 regular legislative session, requires physicians and health care practitioners who use AI for diagnostic purposes – including for any recommendations on a diagnosis or course of treatment based on a patient’s medical records – to, effective Sept. 1:
- Disclose such use of AI to their patients; and
- Review all records created by AI in a manner consistent with medical records standards.
Additionally, entities covered by the bill – businesses, including physician practices, that assemble, collect, analyze, use, evaluate, store, or transmit protected health information – to:
- Automatically allow a minor patient’s parent, guardian, or conservator to obtain “complete and unrestricted access” to the minor’s EHR, unless access to all or part of the record is restricted under state or federal law or by court order, also effective Sept. 1; and
- Physically maintain their EHRs only within the U.S. or a territory of the U.S. and only allow their data to be accessed by those who require the information to perform duties within their scope of their job related to treatment, payment, and other health care operations by Jan. 1, 2026. Covered entities have until Jan. 1, 2026 to ensure compliance relating to EHRs prepared before Sept. 1.
However, Texas physicians are now allowed three days to communicate the results of certain sensitive or serious test results to patients, including minors and their guardians, before they are made available via EHRs thanks to the passage of Senate Bill 922.
SB 1188 also prohibits covered entities from amending on an EHR an individual’s biological sex as recorded by a health care practitioner at birth and documented in the EHR, except to correct a clerical error, or, if the individual is diagnosed with a sexual development disorder, to change the individual’s listed biological sex to the opposite biological sex, in which case, information on the disorder must be also included in the EHR.
SB 1188 states regulatory agencies – including the Texas Medical Board, the Texas Department of Licensing and Regulation, and the Texas Department of Insurance – may take disciplinary action against a covered entity that violates the order three or more times in the same manner. The disciplinary action may include “license, registration, or certification suspension or revocation for a period the agency determines appropriate,” per the law.
Violations of SB 1188 can also result in civil penalties ranging from $5,000 to $250,000 per violation, depending on the violator’s intent and whether the violator used protected health information for financial gain.
Physicians should monitor for future guidance and check with their EHR vendor about compliance, especially as related to where patient data is stored, says Shannon Vogel, the Texas Medical Association’s associate vice president of health information technology.
For more information on health information technology, visit TMA’s related webpage.
Goverment Shutdown: What you Need to Know
With the government shutdown in effect, the Texas Medical Association is in regular communication with federal colleagues at the American Medical Association on the impact to physician practices, as AMA remains in touch with senior officials at the Centers for Medicare & Medicaid Services (CMS).
The volatility in Washington, D.C. could mean the shutdown lasts days to weeks, and TMA will share additional information via Texas Medicine Today as the situation develops. Here is what physicians need to know so far:
Medicare/Medicaid: The CMS contingency plan states that during a lapse in funding, the Medicare program will continue. CMS also says it has sufficient funding for Medicaid to fund the first quarter of 2026 and is maintaining the staff necessary to make payments to eligible states for the Children’s Health Insurance Program.
Medicare Administrative Contractors (MACs) have been instructed to implement a temporary claims hold of 10 business days, which AMA says should have minimal impact on physicians due to the 14-day payment floor. “The hold prevents the need for reprocessing large volumes of claims should Congress act after the statutory expiration date,” states a CMS Medicare Learning Network Connects special edition email newsletter that, as of this writing, had not yet been publicly posted. Physicians may continue to submit claims during this period, but payment will not be released until the hold is lifted. For the latest information, AMA recommends physicians monitor their MAC’s website (Novitas in Texas) and this CMS webpage.
“In the past, Congress generally has restored lapsed policies back to the effective date of the shutdown. During the shutdown, the AMA is monitoring any potential delays in Medicare claims processing or other Medicare payment problems that could result from federal staffing reductions at CMS, including during the shutdown,” said AMA CEO and Executive Vice President John Whyte, MD, MPH.
Telehealth: Physicians who provide telehealth services to fee-for-service Medicare patients should be aware that the Medicare telehealth flexibilities lapsed on Sept. 30 for most care and congressional action is required to restore that waiver. The exceptions are patients being treated for mental health and/or behavioral health disorder (including substance use disorders), stroke, and monthly end-stage renal disease visits for home dialysis. Otherwise, telehealth services are limited to rural areas as they were before the COVID public health emergency, and patients cannot receive telehealth services in their homes. The ability to provide audio-only services to Medicare patients also lapsed, as did the Acute Hospital Care at Home program.
The CMS newsletter suggests “practitioners who choose to perform telehealth services that are not payable by Medicare on or after Oct. 1, 2025, may want to evaluate providing beneficiaries with an Advance Beneficiary Notice of Noncoverage.”
However, AMA notes physicians in certain Medicare Shared Savings Program accountable care organizations can continue to provide and be paid for telehealth services.
Other services: CMS says it is continuing federal insurance marketplace activities, such as eligibility verification. Other nondiscretionary activities including health care fraud and abuse control and Center for Medicare & Medicaid Innovation activities are also continuing.
However, AMA reports that funding extensions for community health centers, the National Health Service Corps, and teaching health centers that operate graduate medical education programs expired on Sept. 30, and the 1.0 work geographic practice cost index floor extension expired on Oct. 1. Additional programs that have lapsed include: special diabetes programs; public health emergency authorities (e.g., Public Health Emergency Fund); increased inpatient hospital payment adjustment for certain low-volume hospitals; the Medicare-Dependent Hospital program; quality measure endorsement, input, and selection; and outreach and assistance for low-income programs (e.g., area agencies on aging).
TMA wants to hear from you. If you or your practice staff experience Medicare payment delays, telehealth obstacles, or other concerns, please let us know through TMA’s Knowledge Center to help inform advocacy.
Amy Lynn Sorrel
Associate Vice President, Editorial Strategy & Programming
Division of Communications and Marketing
Government Shutdown Changes

What has changed due to the Government Shutdown?
It’s pandemic-era flexibilities that will come to an end:
- Geographic restrictions that only permitted telehealth in medically underserved areas
- Requiring the patient to go to an originating site (a health care facility) instead of being in their homes
- Allowing therapists (PTs, OTs, SLPS, audiologists) to perform services via telehealth
Behavioral health via telehealth will still be allowed after September 30th, because Congress passed a law allowing it permanently. It won’t be affected by a government shutdown, if one occurs. The Social Security Act references “mental health” as opposed to “behavioral”.
Quoting the MLN Matters Article on E/M services
MLN006764 September 2025
Telehealth Services
Section 2207 of the Full-Year Continuing Appropriations and Extensions Act, 2025, extended many of these flexibilities through September 30th, 2025. Starting October 1, 2025, the statutory limitations that were in place for Medicare telehealth services before the COVID-19 public health emergency (PHE) will retake effect for most telehealth services.
These include:
- Geographic restrictions
- Location restrictions on where you can provide services
- Limitations on the scope of practitioners who can provide telehealth services
That is, telehealth as we know it to anywhere in the country, in the patient’s home ends. How do you know if you are in an underserved area, and can continue to do telehealth? Quick and easy: could your practice do telehealth before the pandemic? Yes: in all likelihood, you can continue, but remember the patient must go to an originating site, not their homes. Are you in an underserved area? Check here.
At CodingIntel, we have a copy of the CMS telehealth fact sheet from prior to the pandemic. It isn’t up-to-date with the list below, but it will tell you the rules for most practices in the country if a shutdown occurs.
Still allowed are services that weren’t implemented as a result of the pandemic.
eCFR :: 42 CFR 410.78 — Telehealth services.
(iv) The geographic requirements specified in paragraph (b)(4) of this section do not apply to the following telehealth services:
(A) Home dialysis monthly ESRD-related clinical assessment services furnished on or after January 1st, 2019, at an originating site described in paragraphs (b)(3)(vi), (ix), or (x) of this section, in accordance with section 1881(b)(3)(B) of the Act; and
(B) Services furnished on or after January 1st, 2019, for purposes of diagnosis, evaluation, or treatment of symptoms of an acute stroke.
(C) Services furnished on or after July 1st, 2019, to an individual with a substance use disorder diagnosis, for purposes of treatment of a substance use disorder or a co-occurring mental health disorder.
(D) Services furnished on or after January 1st, 2025, for the purposes of diagnosis, evaluation, and/or treatment of a mental health disorder. Payment will not be made for a telehealth service furnished under this paragraph unless the physician or practitioner has furnished an item or service in person, without the use of telehealth, for which Medicare payment was made (or would have been made if the patient were entitled to, or enrolled for, Medicare benefits at the time the item or service is furnished) within 6 months prior to the initial telehealth service and within 6 months of any subsequent telehealth service.
Betsy
Sorry POST Missing
POET ask you to forgive us. The post in the “Latest Post” email titled “If you think 2024 was good” had to be taken down. The video of October 2024 festivities was causing a gliche.
BUT….. If you like old abandoned hospitals……
Come see 2025
UHC “Check by Member” Authorization Tool
UHC says they have a smarter way to check prior authorization requirements.
Our upgraded Check by Member tool is now the most accurate and reliable way to confirm prior authorization requirements.
- Personalized results based on member-specific data
- Same trusted source as our phone advocates
- Instant answers with no hold time

Beware of Calls Appearing to Come From TDLR
“We’ve been hearing from licensees that some of you have received suspicious phone calls that appear to come from the TDLR Customer Service line (512-463-6599).
These calls usually come from someone claiming to be a TDLR investigator who says there’s an issue with the TDLR license or file. Other calls have claimed that the person receiving the call is a victim of identity theft and that a criminal case has been filed against them. Other calls have claimed that the FBI is investigating the licensee.
Please know this: we won’t call you to tell you that your license is suspended or that you’re being investigated or ask you for money.
If you receive a phone call that appears to come from TDLR but you haven’t called or emailed us first – and if the caller is asking for personal information or requests payment – please don’t provide any information or payment. Call TDLR first to confirm whether we actually called you – because we probably didn’t.”
CMS Releases 2024 MIPS Scores

The Centers for Medicare & Medicaid Services (CMS) has released MIPS performance feedback and final scores for the 2024 performance year. Sign in to the Quality Payment Program (QPP) website using your Health Care Quality Information Systems (HCQIS) Access Roles and Profile (HARP) system credentials to view your feedback from CMS. The targeted review period will be open for approximately 60 days, beginning with the release of final scores and closing 30 days after the release of MIPS payment adjustments that CMS plans to announce in one month.
NEW TMB Website is Live!
The Texas Medical Board (TMB) is excited to announce that their redesigned website is now live!
They have made updates to improve our experience and ensure easier access to information and services but don’t worry, all existing systems, including My TMB, remain unchanged and fully accessible.
What’s New:
- New Website & Email Addresses: Our website has moved from tmb.state.tx.us to www.tmb.texas.gov. TMB staff and board member email addresses have also changed to the @tmb.texas.gov domain, aligning with other Texas state agencies.
- Fresh Look & Improved Navigation: The updated design features a cleaner, more modern layout with streamlined navigation to help you find what you need more easily.
Tip: Don’t forget to update any bookmarks or saved links to our new website: www.tmb.texas.gov
If you have questions about finding information on the new site, please contact the TMB Customer Service team at (512) 305-7030 or, within Texas, (800) 248-4062. You may also send an email to [email protected]
Physician NPI Revocations
The US Department of Health and Human Services will close six of its 10 regional counsel offices in 2025, raising concerns about delays, due process and physician appeals of NPI revocations.
Why does this matter to doctors? First, and most obviously, many enforcement actions could be slowed to a crawl, which would at first blush, seem to be a good thing for doctors.
However, there is a second problem. Some actions, such as “revocations” of NPI numbers, can be performed administratively, without any legal due process whatsoever. When this happens, providers may receive a letter informing them that their NPI number has been suspended or revoked together with a statement of the provider’s “appeal” rights.
Although doctors must appeal immediately, an appeal cannot go forward without lawyers from the OGC to appear on behalf of HHS. What happens if there aren’t any?
I tried a case in 2021 with a fully staffed OGC. First, to the Department Appeals Board and then to an ALJ in Washington D.C. My client’s offense? “Failure to produce medical records.” HHS administratively revoked my client’s NPI for 10 years.
While the DAB lowered the revocation to 3 years, when we appealed to the ALJ, we didn’t get an answer for two more years, during which time, the doctor was not allowed to submit any claims to CMS. And this was with a fully staffed OGC. Can you imagine what will happen with 6 of 10 offices closed?
A physician could continue to see patients, during the appeal of a suspension or revocation, but ordinarily must hold the claims until his NPI number suspension is reversed. Which, as I noted, took me two years to push an appeal through, when the OGC was fully staffed.
I have no idea how anyone is going to get any relief, if no one can have a hearing. Meaning, “due process” no longer exists in NPI revocations.
Martin Merritt is a health lawyer and health care litigator at Martin Merritt PLLC, as well as past president of the Texas Health Lawyers Association and past chairman of the Dallas Bar Association Health Law Section. He can be reached at [email protected].
Recent Comments